Analysis of pulmonary features and treatment approaches in the COPA syndrome
- PMID: 29977900
- PMCID: PMC6019741
- DOI: 10.1183/23120541.00017-2018
Analysis of pulmonary features and treatment approaches in the COPA syndrome
Abstract
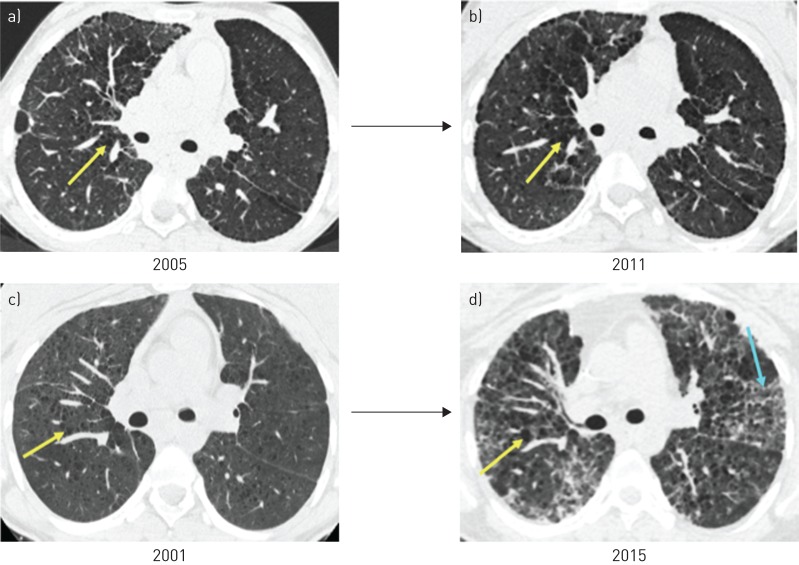
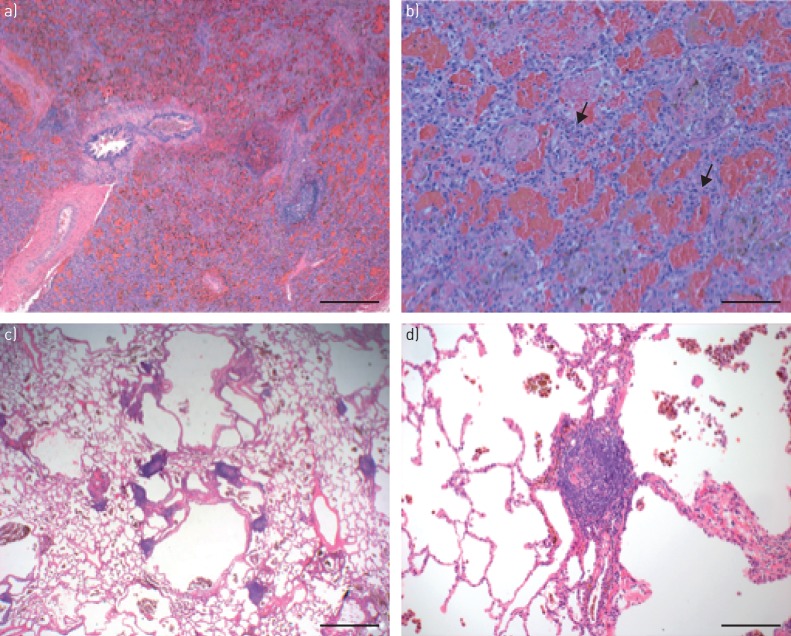
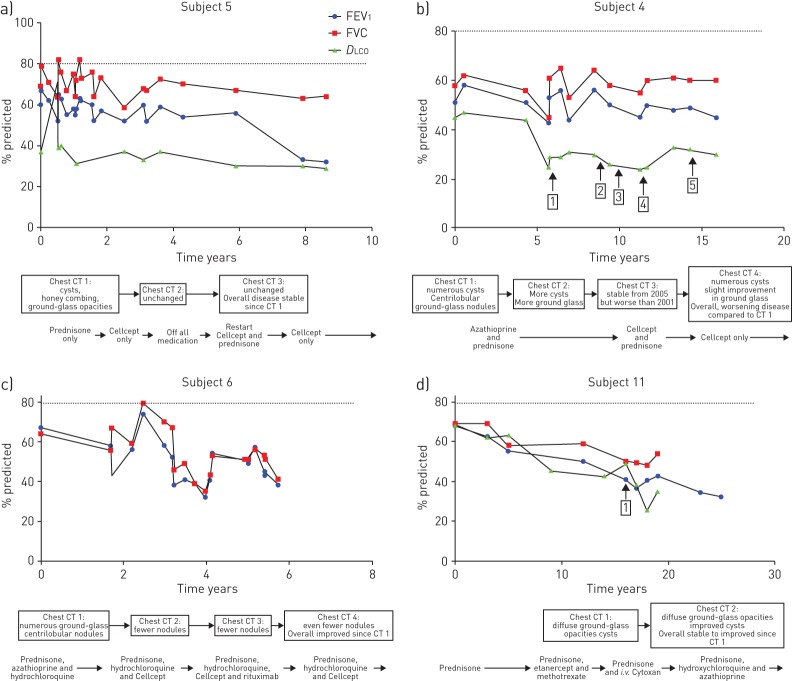
The COPA syndrome is a monogenic, autoimmune lung and joint disorder first identified in 2015. This study sought to define the main pulmonary features of the COPA syndrome in an international cohort of patients, analyse patient responses to treatment and highlight when genetic testing should be considered. We established a cohort of subjects (N=14) with COPA syndrome seen at multiple centres including the University of California, San Francisco, CA, USA. All subjects had one of the previously established mutations in the COPA gene, and had clinically apparent lung disease and arthritis. We analysed cohort characteristics using descriptive statistics. All subjects manifested symptoms before the age of 12 years, had a family history of disease, and developed diffuse parenchymal lung disease and arthritis. 50% had diffuse alveolar haemorrhage. The most common pulmonary findings included cysts on chest computed tomography and evidence of follicular bronchiolitis on lung biopsy. All subjects were positive for anti-neutrophil cytoplasmic antibody, anti-nuclear antibody or both and 71% of subjects had rheumatoid factor positivity. All subjects received immunosuppressive therapy. COPA syndrome is an autoimmune disorder defined by diffuse parenchymal lung disease and arthritis. We analysed an international cohort of subjects with genetically confirmed COPA syndrome and found that common pulmonary features included cysts, follicular bronchiolitis and diffuse alveolar haemorrhage. Common extrapulmonary features included early age of onset, family history of disease, autoantibody positivity and arthritis. Longitudinal data demonstrated improvement on chest radiology but an overall decline in pulmonary function despite chronic treatment.
Conflict of interest statement
Conflict of interest: None declared
Figures