

Use of over-the-scope-clip (OTSC) improves outcomes of high-risk adverse outcome (HR-AO) non-variceal upper gastrointestinal bleeding (NVUGIB)
- PMID: 29977995
- PMCID: PMC6031436
- DOI: 10.1055/a-0614-2390
Use of over-the-scope-clip (OTSC) improves outcomes of high-risk adverse outcome (HR-AO) non-variceal upper gastrointestinal bleeding (NVUGIB)
Abstract
Background and study aims: Endoscopic treatment of non-variceal upper gastrointestinal bleeding (NVUGIB) with high-risk adverse outcome (HR-AO) features has a high risk of failure. We studied the safety and efficacy of over-the-scope clips (OTSC) to treat these lesions.
Patients and methods: We included patients who were treated using OTSC for NVUGIB from January 2015 to October 2017. We studied rebleeding and mortality rates and used the Rockall data and our institution's prior data for comparison. We used descriptive and chi-square statistics.
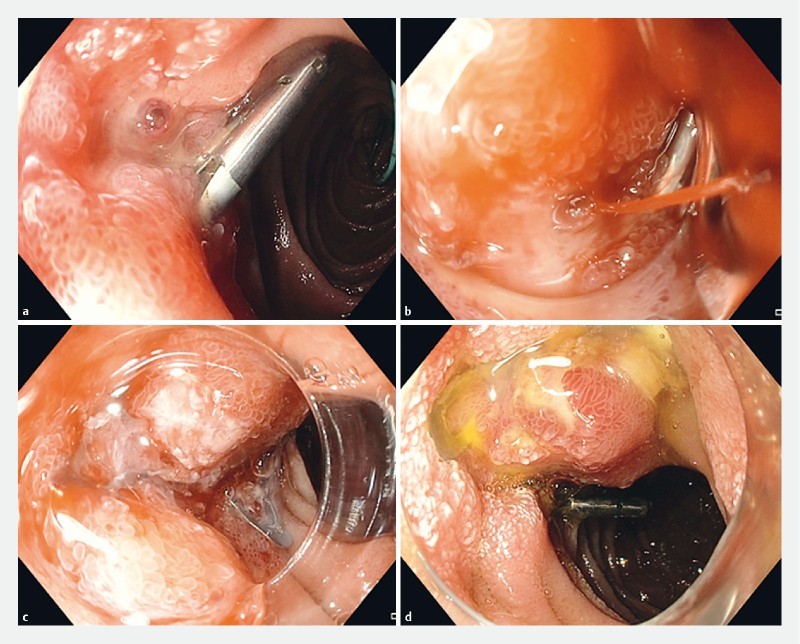
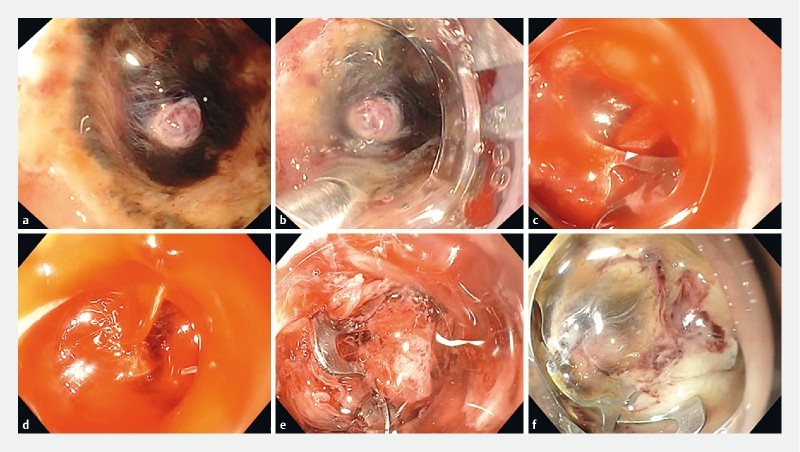
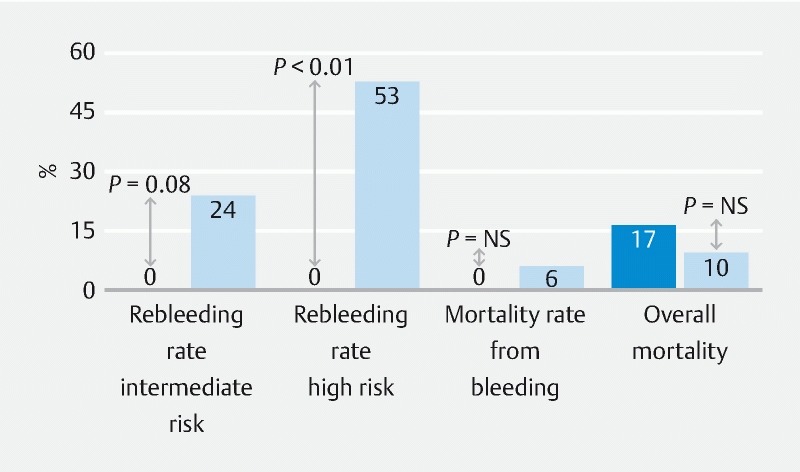
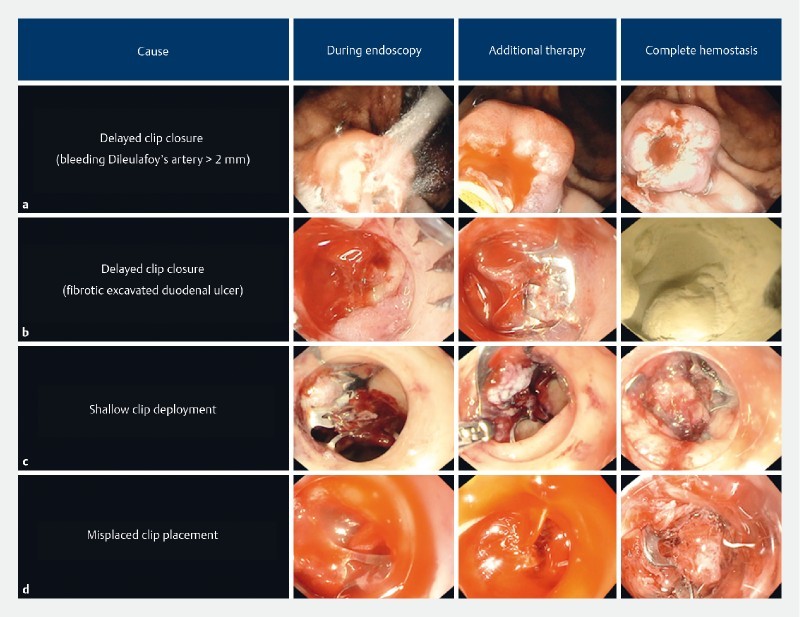
Results: We studied 18 patients with 19 bleeding lesions: 9 (47 %) duodenal ulcers, 4 (21 %) Dieulafoy's lesion, 3 (16 %) gastric ulcer, and 3 (16 %) bleeding after gastric biopsy, gastric polypectomy and endoscopic ultrasound-guided fine-needle aspiration of peri-gastric mass. We applied OTSC as the first-line treatment in 10 (53 %) and as the second-line treatment in 9 (47 %) bleeding lesions. Continued bleeding after OTSC occurred in six patients, but we treated it successfully and achieved complete hemostasis in all patients. We found OTSC use significantly decreased (0 % vs. 53 %, P < 0.01) and reduced (0 % vs. 24 %, P = 0.08) the rebleeding rate in our high-risk (RS ≥ 8) and intermediate-risk (RS = 4 - 7) Rockall score patients as compared to the rates reported by the Rockall study, respectively. When compared to our institution's prior study, we found a decrease in the rebleeding rate with OTSC (0 % vs. 21 %, P = 0.06) in our intermediate-to-high risk Rockall score patients (RS ≥ 4). There was no difference in mortality rates as compared to both control studies.
Conclusion: Use of OTSC is safe, efficacious and appears superior to standard treatment for HR-AO NVUGIB. OTSC should be considered as first-line treatment for HR-AO bleeding.
Conflict of interest statement
Figures
Similar articles
-
Multicenter evaluation of first-line endoscopic treatment with the OTSC in acute non-variceal upper gastrointestinal bleeding and comparison with the Rockall cohort: the FLETRock study.Surg Endosc. 2018 Jan;32(1):307-314. doi: 10.1007/s00464-017-5678-7. Epub 2017 Jun 27. Surg Endosc. 2018. PMID: 28656336
-
Over-the-scope clip vs epinephrine with clip for first-line hemostasis in non-variceal upper gastrointestinal bleeding: a propensity score match analysis.Endosc Int Open. 2020 Jan;8(1):E50-E58. doi: 10.1055/a-1005-6401. Epub 2020 Jan 8. Endosc Int Open. 2020. PMID: 31921984 Free PMC article.
-
Over-the-Scope Clip Applications as First-Line Therapy in the Treatment of Upper Non-variceal Gastrointestinal Bleeding, Perforations, and Fistulas.Front Med (Lausanne). 2022 Feb 15;9:753956. doi: 10.3389/fmed.2022.753956. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35242770 Free PMC article.
-
Over-the-Scope Clips Versus Standard Endoscopic Treatment for First Line Therapy of Non-variceal Upper Gastrointestinal Bleeding: Systematic Review and Meta-Analysis.Dig Dis Sci. 2023 Jun;68(6):2518-2530. doi: 10.1007/s10620-023-07888-3. Epub 2023 Mar 21. Dig Dis Sci. 2023. PMID: 36943590
-
Over-the-scope clips for Nonvariceal upper gastrointestinal bleeding: a systematic review and meta-analysis of randomized studies.Postgrad Med J. 2025 Mar 16;101(1194):351-359. doi: 10.1093/postmj/qgae155. Postgrad Med J. 2025. PMID: 39500365
Cited by
-
Adverse events associated with the gold probe and the injection gold probe devices used for endoscopic hemostasis: A MAUDE database analysis.World J Gastrointest Endosc. 2024 Jan 16;16(1):37-43. doi: 10.4253/wjge.v16.i1.37. World J Gastrointest Endosc. 2024. PMID: 38313458 Free PMC article.
-
Over-the-Scope Clip to the Rescue! A Novel Tool for Refractory Acute Nonvariceal Upper Gastrointestinal Hemorrhage.Case Rep Gastroenterol. 2020 May 12;14(2):261-270. doi: 10.1159/000507610. eCollection 2020 May-Aug. Case Rep Gastroenterol. 2020. PMID: 32518537 Free PMC article.
-
Endoscopic clipping in non-variceal upper gastrointestinal bleeding treatment.Clin Endosc. 2022 May;55(3):339-346. doi: 10.5946/ce.2021.249. Epub 2022 Apr 28. Clin Endosc. 2022. PMID: 35534934 Free PMC article. Review.
-
Clinical efficacy of the over-the-scope clip device: A systematic review.World J Gastroenterol. 2020 Jun 28;26(24):3495-3516. doi: 10.3748/wjg.v26.i24.3495. World J Gastroenterol. 2020. PMID: 32655272 Free PMC article.
-
Over-the-scope clip as a rescue treatment for massive bleeding due to Dieulafoy lesion at the colorectal anastomosis: A case report.Medicine (Baltimore). 2024 Apr 19;103(16):e37871. doi: 10.1097/MD.0000000000037871. Medicine (Baltimore). 2024. PMID: 38640308 Free PMC article.
References
-
- Barkun A N, Bardou M, Kuipers E J et al.International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med. 2010;152:101–113. - PubMed
-
- Gralnek I M, Dumonceau J M, Kuipers E J et al.Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2015;47:a1–46. - PubMed
-
- Laine L, Jensen D M. Management of patients with ulcer bleeding. Am J Gastroenterol. 2012;107:345–360. - PubMed
-
- Barkun A N, Martel M, Toubouti Y et al.Endoscopic hemostasis in peptic ulcer bleeding for patients with high-risk lesions: a series of meta-analyses. Gastrointest Endosc. 2009;69:786–799. - PubMed
-
- Kato M, Jung Y, Gromski M A et al.Prospective, randomized comparison of 3 different hemoclips for the treatment of acute upper GI hemorrhage in an established experimental setting. Gastrointest Endosc. 2012;75:3–10. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources