

Metastatic and triple-negative breast cancer: challenges and treatment options
- PMID: 29978332
- PMCID: PMC6133085
- DOI: 10.1007/s13346-018-0551-3
Metastatic and triple-negative breast cancer: challenges and treatment options
Abstract
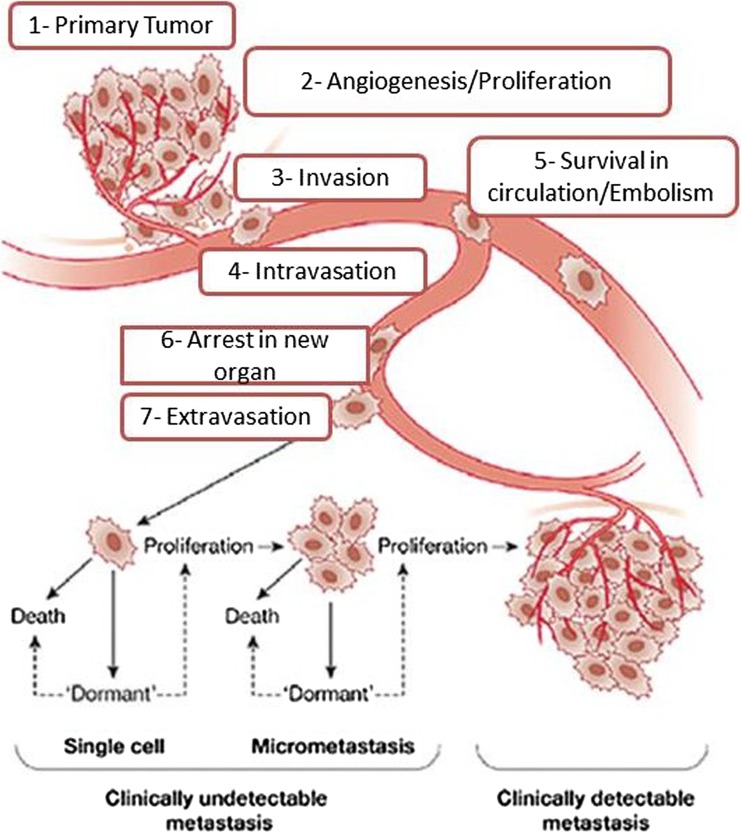
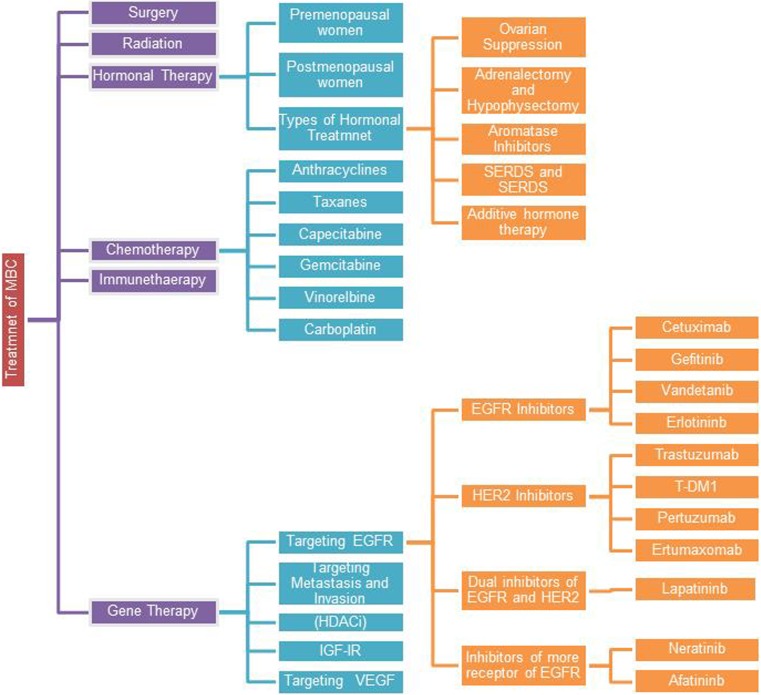
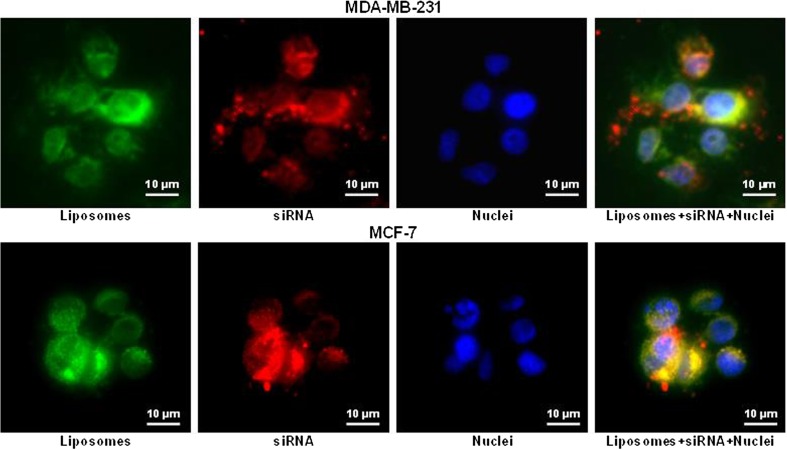
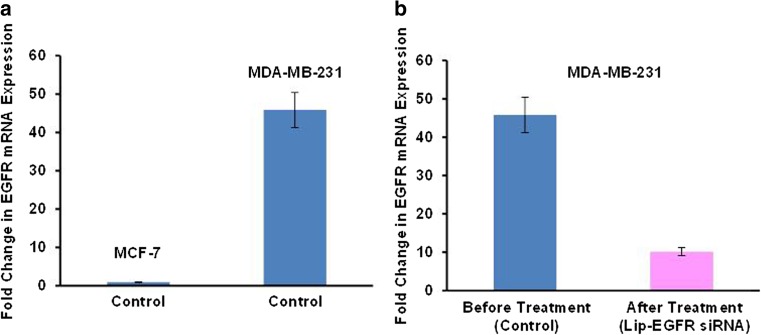
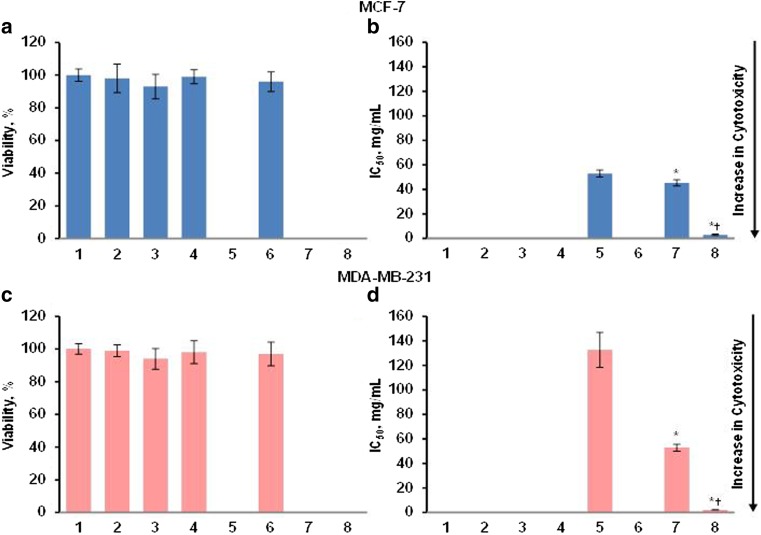
The major current conventional types of metastatic breast cancer (MBC) treatments include surgery, radiation, hormonal therapy, chemotherapy, or immunotherapy. Introducing biological drugs, targeted treatment and gene therapy can potentially reduce the mortality and improve the quality of life in patients with MBC. However, combination of several types of treatment is usually recommended. Triple negative breast cancer (TNBC) accounts for 10-20% of all cases of breast carcinoma and is characterized by the low expression of progesterone receptor (PR), estrogen receptor (ER), and human epidermal growth factor receptor 2 (HER2). Consequently, convenient treatments used for MBC that target these receptors are not effective for TNBC which therefore requires special treatment approaches. This review discusses the occurrence of MBC, the prognosis and predictive biomarkers of MBC, and focuses on the novel advanced tactics for treatment of MBC and TNBC. Nanotechnology-based combinatorial approach for the suppression of EGFR by siRNA and gifitinib is described.
Keywords: Combinatorial treatment of breast cancer; EGFR; Gefitinib; Liposomes; siRNA.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Animal studies
All institutional and national guidelines for the care and use of laboratory animals were followed.
Figures
References
-
- Lyden D, Welch DR, Psaila B. Cancer metastasis: biologic basis and therapeutics. Cambridge University Press; 2011.
-
- Gerratana L, Fanotto V, Bonotto M, Bolzonello S, Minisini AM, Fasola G, et al. Pattern of metastasis and outcome in patients with breast cancer. Clinical & Experimental Metastasis. 2015;32:125–133. - PubMed
-
- Kang Y, Siegel PM, Shu W, Drobnjak M, Kakonen SM, Cordón-Cardo C, et al. A multigenic program mediating breast cancer metastasis to bone. Cancer Cell. 2003;3:537–549. - PubMed
-
- Mansel WG, R. E., Fodstad, O. & Jiang. Metastasis of breast cancer. Netherland: Springer; 2007.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
