

Variation in Sedation and Neuromuscular Blockade Regimens on Outcome After Cardiac Arrest
- PMID: 29979225
- PMCID: PMC6138551
- DOI: 10.1097/CCM.0000000000003301
Variation in Sedation and Neuromuscular Blockade Regimens on Outcome After Cardiac Arrest
Abstract
Objectives: Sedation and neuromuscular blockade protocols in patients undergoing targeted temperature management after cardiac arrest address patient discomfort and manage shivering. These protocols vary widely between centers and may affect outcomes.
Design: Consecutive patients admitted to 20 centers after resuscitation from cardiac arrest were prospectively entered into the International Cardiac Arrest Registry between 2006 and 2016. Additional data about each center's sedation and shivering management practice were obtained via survey. Sedation and shivering practices were categorized as escalating doses of sedation and minimal or no neuromuscular blockade (sedation and shivering practice 1), sedation with continuous or scheduled neuromuscular blockade (sedation and shivering practice 2), or sedation with as-needed neuromuscular blockade (sedation and shivering practice 3). Good outcome was defined as Cerebral Performance Category score of 1 or 2. A logistic regression hierarchical model was created with two levels (patient-level data with standard confounders at level 1 and hospitals at level 2) and sedation and shivering practices as a fixed effect at the hospital level. The primary outcome was dichotomized Cerebral Performance Category at 6 months.
Setting: Cardiac arrest receiving centers in Europe and the United states from 2006 to 2016 PATIENTS:: Four-thousand two-hundred sixty-seven cardiac arrest patients 18 years old or older enrolled in the International Cardiac Arrest Registry.
Interventions: None.
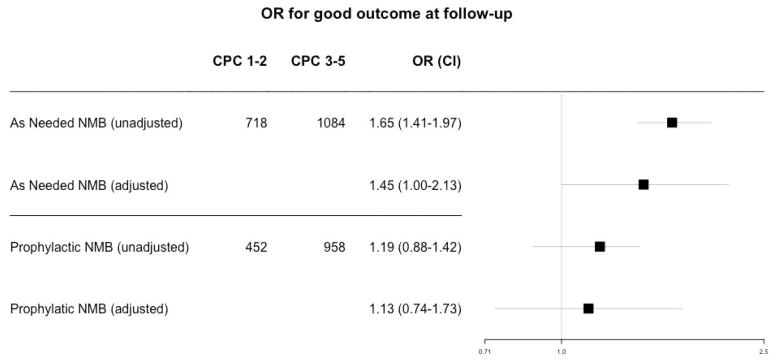
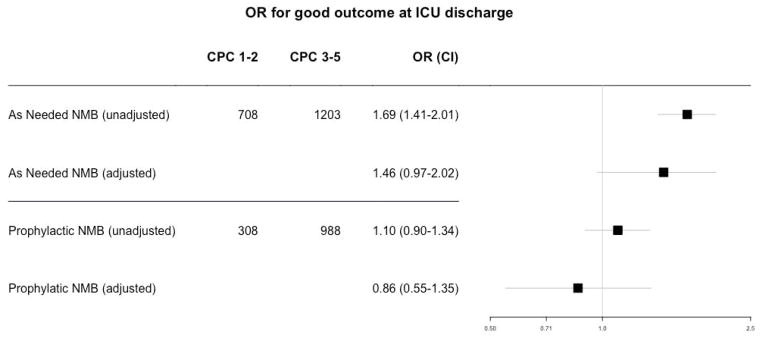
Measurements and main results: The mean age was 62 ± 15 years, 36% were female, 77% out-of-hospital arrests, and mean ischemic time was 24 (± 18) minutes. Adjusted odds ratio (for age, return of spontaneous circulation, location of arrest, witnessed, initial rhythm, bystander cardiopulmonary resuscitation, defibrillation, medical history, country, and size of hospital) was 1.13 (0.74-1.73; p = 0.56) and 1.45 (1.00-2.13; p = 0.046) for sedation and shivering practice 2 and sedation and shivering practice 3, respectively, referenced to sedation and shivering practice 1.
Conclusion: Cardiac arrest patients treated at centers using as-needed neuromuscular blockade had increased odds of good outcomes compared with centers using escalating sedation doses and avoidance of neuromuscular blockade, after adjusting for potential confounders. These findings should be further investigated in prospective studies.
Figures
Comment in
-
Neuromuscular Blockade in Targeted Temperature Management: Giving More or Giving Less?Crit Care Med. 2018 Oct;46(10):1714-1715. doi: 10.1097/CCM.0000000000003323. Crit Care Med. 2018. PMID: 30216314 No abstract available.
References
-
- Chamorro C, Borrallo JM, Romera MA, et al. Anesthesia and analgesia protocol during therapeutic hypothermia after cardiac arrest: a systematic review. Anesthesia and analgesia. 2010;110(5):1328–1335. - PubMed
-
- Choi HA, Ko SB, Presciutti M, et al. Prevention of shivering during therapeutic temperature modulation: the Columbia anti-shivering protocol. Neurocritical care. 2011;14(3):389–394. - PubMed
-
- May TL, Seder DB, Fraser GL, et al. Moderate-Dose Sedation and Analgesia During Targeted Temperature Management After Cardiac Arrest. Neurocritical care. 2014 - PubMed
-
- Wong GC, van Diepen S, Ainsworth C, et al. Canadian Cardiovascular Society/Canadian Cardiovascular Critical Care Society/Canadian Association of Interventional Cardiology Position Statement on the Optimal Care of the Postarrest Patient. The Canadian journal of cardiology. 2017;33(1):1–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
