

Neuroimaging Correlates of Periodic Discharges
- PMID: 29979286
- PMCID: PMC9371611
- DOI: 10.1097/WNP.0000000000000466
Neuroimaging Correlates of Periodic Discharges
Abstract
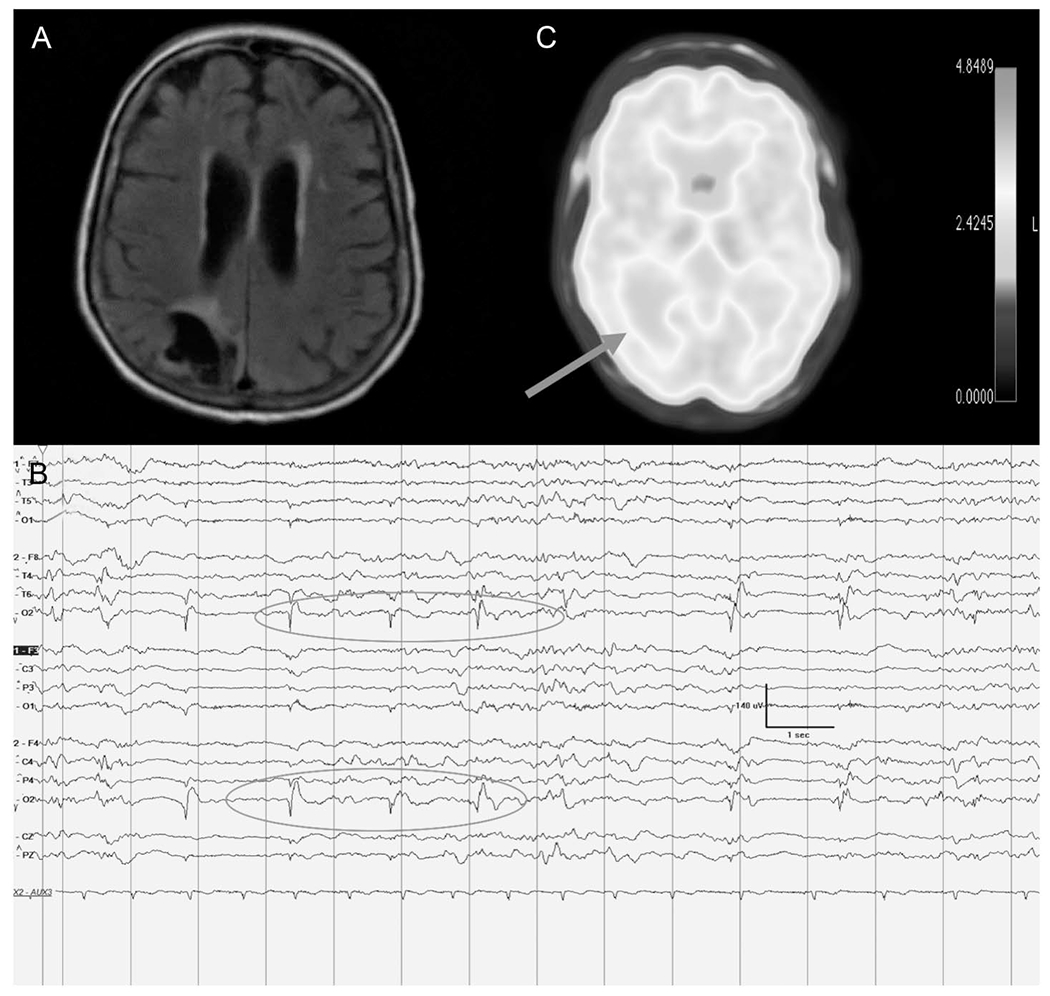
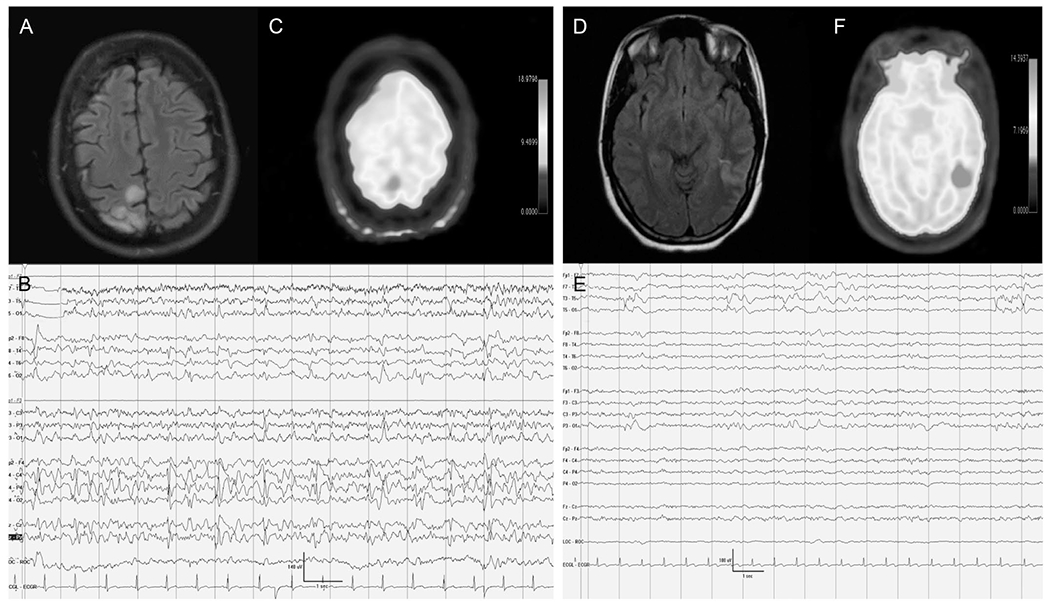
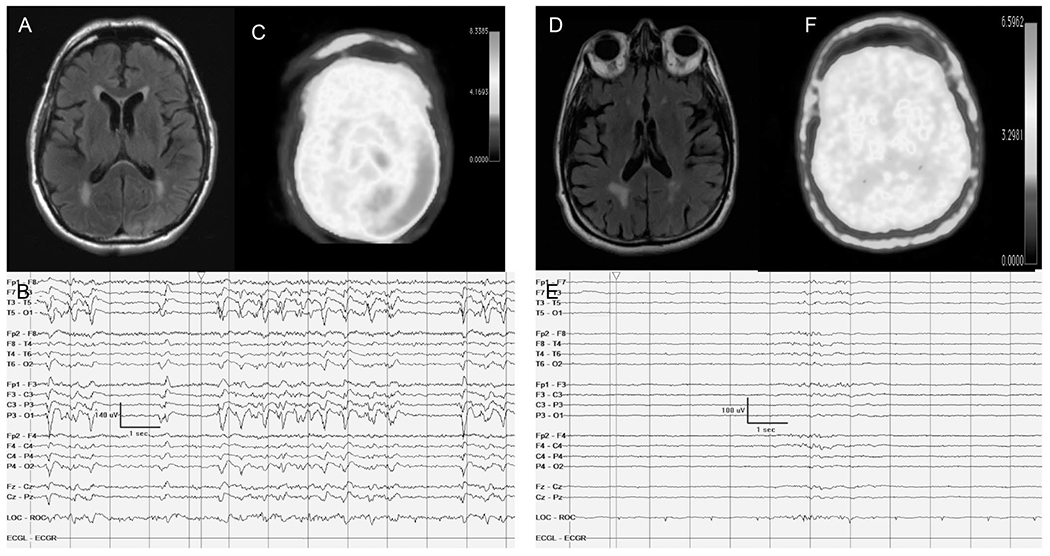
Despite being first described over 50 years ago, periodic discharges continue to generate controversy as to whether they are always, sometimes, or never "ictal." Investigators and clinicians have proposed adjunctive markers to help clarify this distinction-in particular measures of perfusion and metabolism. Here, we review the growing number of neuroimaging studies using Fluorodeoxyglucose-PET, MRI diffusion, Magnetic resonance perfusion, Single Photon Emission Computed Tomography, and Magnetoencepgalography to gain further insight into the physiology and clinical significance of periodic discharges. To date, however, no definitive consensus exists regarding the features of periodic discharges that warrant treatment intensification. However, an emerging consilience among neuroimaging modalities suggests that periodic discharges can induce a hyperexcitatory state with associated hypermetabolism and hyperperfusion, which may result in local metabolic failure.
Conflict of interest statement
The authors have no funding or conflicts of interest to disclose.
Figures
Similar articles
-
Approach to Managing Periodic Discharges.J Clin Neurophysiol. 2018 Jul;35(4):309-313. doi: 10.1097/WNP.0000000000000464. J Clin Neurophysiol. 2018. PMID: 29979289 Review.
-
SPECT-negative SIRPIDs argues against treatment as seizures.J Clin Neurophysiol. 2011 Oct;28(5):493-6. doi: 10.1097/WNP.0b013e318231c00a. J Clin Neurophysiol. 2011. PMID: 21946363
-
The EEG Ictal-Interictal Continuum-A Metabolic Roar But a Whimper of a Functional Outcome.Epilepsy Curr. 2019 Jul-Aug;19(4):234-236. doi: 10.1177/1535759719855968. Epub 2019 Jun 14. Epilepsy Curr. 2019. PMID: 31198061 Free PMC article.
-
Lateralized Periodic Discharges: Which patterns are interictal, ictal, or peri-ictal?Clin Neurophysiol. 2021 Jul;132(7):1593-1603. doi: 10.1016/j.clinph.2021.04.003. Epub 2021 Apr 27. Clin Neurophysiol. 2021. PMID: 34034086 Review.
-
Tonic seizures of Lennox-Gastaut syndrome: periictal single-photon emission computed tomography suggests a corticopontine network.Epilepsia. 2013 Dec;54(12):2151-7. doi: 10.1111/epi.12398. Epub 2013 Oct 10. Epilepsia. 2013. PMID: 24117046
Cited by
-
Electrographic Seizures in the Critically Ill.Neurol Clin. 2022 Nov;40(4):907-925. doi: 10.1016/j.ncl.2022.03.015. Epub 2022 Sep 28. Neurol Clin. 2022. PMID: 36270698 Free PMC article. Review.
-
Critical care EEG standardized nomenclature in clinical practice: Strengths, limitations, and outlook on the example of prognostication after cardiac arrest.Clin Neurophysiol Pract. 2021 Apr 25;6:149-154. doi: 10.1016/j.cnp.2021.03.002. eCollection 2021. Clin Neurophysiol Pract. 2021. PMID: 35112033 Free PMC article. Review.
-
The role of EEG and neuroimaging in the diagnosis of non-convulsive status epilepticus in Subacute Encephalopathy with Seizures in Alcoholics (SESA syndrome): a case report and overview of the literature.Neurol Sci. 2024 Oct;45(10):5053-5062. doi: 10.1007/s10072-024-07609-2. Epub 2024 May 27. Neurol Sci. 2024. PMID: 38802690 Review.
-
Can Spectral Power Be Used as a Candidate Seizure Marker of the Periodic Discharges Pattern?Front Neurol. 2021 Jun 14;12:642669. doi: 10.3389/fneur.2021.642669. eCollection 2021. Front Neurol. 2021. PMID: 34194380 Free PMC article.
-
Periodic discharges in veterinary electroencephalography-A visual review.Front Vet Sci. 2023 Jan 26;10:1037404. doi: 10.3389/fvets.2023.1037404. eCollection 2023. Front Vet Sci. 2023. PMID: 36777678 Free PMC article. Review.
References
-
- Orta DS, Chiappa KH, Quiroz AZ, Costello DJ, Cole AJ. Prognostic implications of periodic epileptiform discharges. Arch Neurol. 2009;66:985–991. - PubMed
-
- Walsh JM, Brenner RP. Periodic lateralized discharges-long term outcome in adults. Epilepsia. 1987;28:533–536. - PubMed
-
- Walton NY, Treiman DM. Response of status epilepticus induced by lithium and pilocarpine to treatment with diazepam. Exp Nerurol. 1988;101:267–275. - PubMed
-
- Leitinger M, Trinka E, Gardella E, et al. Diagnostic accuracy of the Salzburg EEG criteria for non-convulsive status epilepticus: a retrospective study. Lancet Neurol. 2016;10:1054–1062. - PubMed
-
- Trinka E, Cock H, Hesdorffer D, et al. A definition and classification of status epilepticus-report of the ILAE task force on classification of status epilepticus. Epilepsia. 2015;56:1515–1523. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
