

Feasibility of Diffusion Tensor and Morphologic Imaging of Peripheral Nerves at Ultra-High Field Strength
- PMID: 29979328
- PMCID: PMC6221405
- DOI: 10.1097/RLI.0000000000000492
Feasibility of Diffusion Tensor and Morphologic Imaging of Peripheral Nerves at Ultra-High Field Strength
Abstract
Objectives: The aim of this study was to describe the development of morphologic and diffusion tensor imaging sequences of peripheral nerves at 7 T, using carpal tunnel syndrome (CTS) as a model system of focal nerve injury.
Materials and methods: Morphologic images were acquired at 7 T using a balanced steady-state free precession sequence. Diffusion tensor imaging was performed using single-shot echo-planar imaging and readout-segmented echo-planar imaging sequences. Different acquisition and postprocessing methods were compared to describe the optimal analysis pipeline. Magnetic resonance imaging parameters including cross-sectional areas, signal intensity, fractional anisotropy (FA), as well as mean, axial, and radial diffusivity were compared between patients with CTS (n = 8) and healthy controls (n = 6) using analyses of covariance corrected for age (significance set at P < 0.05). Pearson correlations with Bonferroni correction were used to determine association of magnetic resonance imaging parameters with clinical measures (significance set at P < 0.01).
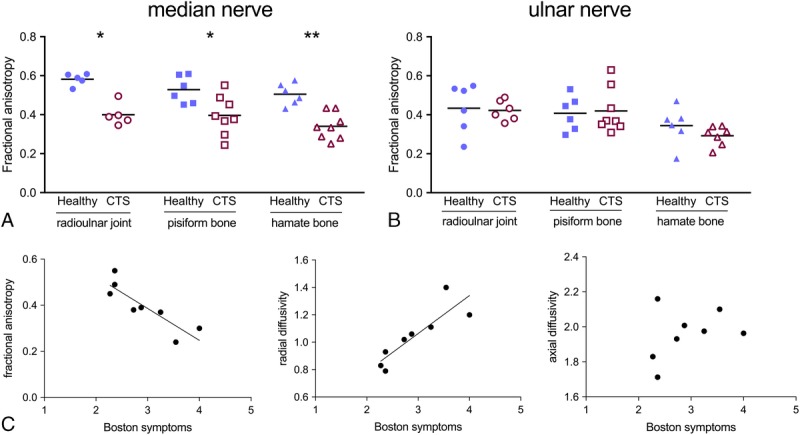
Results: The 7 T acquisitions with high in-plane resolution (0.2 × 0.2mm) afforded detailed morphologic resolution of peripheral nerve fascicles. For diffusion tensor imaging, single-shot echo-planar imaging was more efficient than readout-segmented echo-planar imaging in terms of signal-to-noise ratio per unit scan time. Distortion artifacts were pronounced, but could be corrected during postprocessing. Registration of FA maps to the morphologic images was successful. The developed imaging and analysis pipeline identified lower median nerve FA (pisiform bone, 0.37 [SD 0.10]) and higher radial diffusivity (1.08 [0.20]) in patients with CTS compared with healthy controls (0.53 [0.06] and 0.78 [0.11], respectively, P < 0.047). Fractional anisotropy and radial diffusivity strongly correlated with patients' symptoms (r = -0.866 and 0.866, respectively, P = 0.005).
Conclusions: Our data demonstrate the feasibility of morphologic and diffusion peripheral nerve imaging at 7 T. Fractional anisotropy and radial diffusivity were found to be correlates of symptom severity.
Conflict of interest statement
Conflicts of interest and sources of funding: none declared.
Figures





References
-
- Filler AG, Howe FA, Hayes CE, et al. Magnetic resonance neurography. Lancet. 1993;341:659–661. - PubMed
-
- Kollmer J, Bendszus M, Pham M. MR neurography: diagnostic imaging in the PNS. Clin Neuroradiol. 2015;25(suppl 2):283–289. - PubMed
-
- Chhabra A, Madhuranthakam AJ, Andreisek G. Magnetic resonance neurography: current perspectives and literature review. Eur Radiol. 2018;28:698–707. - PubMed
-
- Gambarota G, Veltien A, Klomp D, et al. Magnetic resonance imaging and T2 relaxometry of human median nerve at 7 Tesla. Muscle Nerve. 2007;36:368–373. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
