

Implementing evidence-based practices in the care of infants with bronchiolitis in Australasian acute care settings: study protocol for a cluster randomised controlled study
- PMID: 29980177
- PMCID: PMC6035428
- DOI: 10.1186/s12887-018-1187-7
Implementing evidence-based practices in the care of infants with bronchiolitis in Australasian acute care settings: study protocol for a cluster randomised controlled study
Abstract
Background: Bronchiolitis is the most common reason for admission to hospital for infants less than one year of age. Although management is well defined, there is substantial variation in practice, with infants receiving ineffective therapies or management. This study will test the effectiveness of tailored, theory informed knowledge translation (KT) interventions to decrease the use of five clinical therapies or management processes known to be of no benefit, compared to usual dissemination practices in infants with bronchiolitis. The primary objective is to establish whether the KT interventions are effective in increasing compliance to five evidence based recommendations in the first 24 h following presentation to hospital. The five recommendations are that infants do not receive; salbutamol, antibiotics, glucocorticoids, adrenaline, or a chest x-ray.
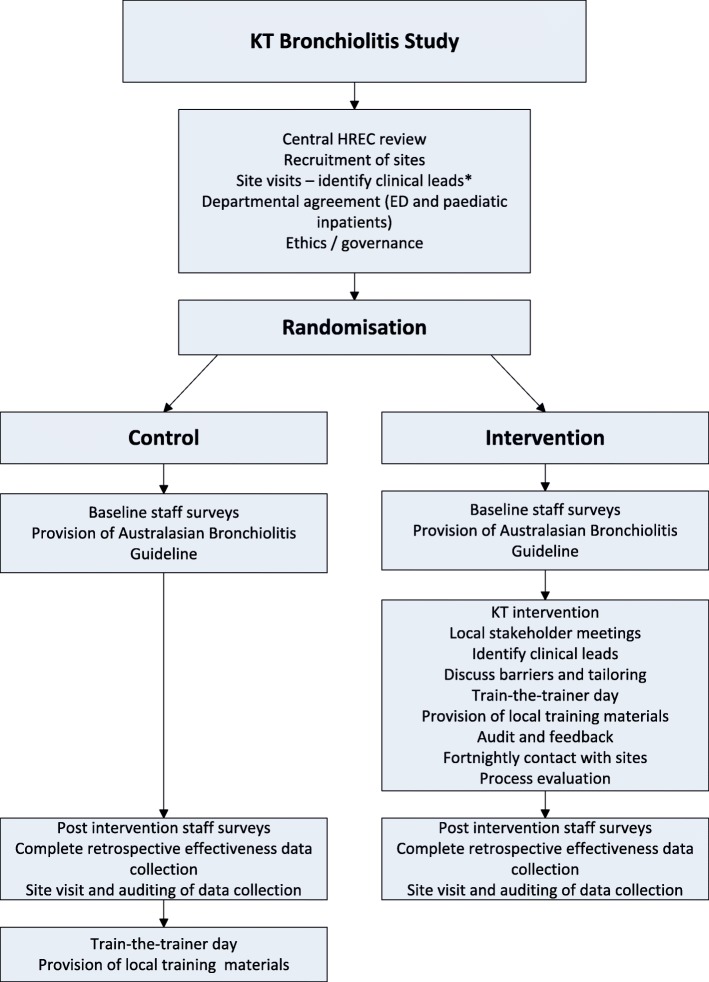
Methods/design: This study is designed as a cluster randomised controlled trial. We will recruit 24 hospitals in Australia and New Zealand, stratified by country and provision of tertiary or secondary paediatric care. Hospitals will be randomised to either control or intervention groups. Control hospitals will receive a copy of the recent Australasian Bronchiolitis Guideline. Intervention hospitals will receive KT interventions informed by a qualitative analysis of factors influencing clinician care of infants with bronchiolitis. Key interventions include, local stakeholder meetings, identifying medical and nursing clinical leads in both emergency departments and paediatric inpatient areas who will attend a single education train-the-trainer day to then deliver standardised staff education with the training materials provided and coordinate audit and feedback reports locally over the study period. Data will be extracted retrospectively for three years prior to the study intervention year, and for seven months of the study intervention year bronchiolitis season following intervention delivery to determine compliance with the five evidence-based recommendations. Data will be collected to assess fidelity to the implementation strategies and to facilitate an economic evaluation.
Discussion: This study will contribute to the body of knowledge to determine the effectiveness of tailored, theory informed interventions in acute care paediatric settings, with the aim of reducing the evidence to practice gaps in the care of infants with bronchiolitis.
Trial registration: Australian New Zealand Clinical Trials Registry ACTRN12616001567415 (retrospectively registered on 14 November 2016).
Keywords: Acute care; Bronchiolitis; Cluster trial; Implementation; Knowledge translation strategies.
Conflict of interest statement
Ethics approval and consent to participate
This study has undergone ethics review and been approved by the Royal Children’s Hospital Human Research Ethics Committee (EC00238), Australia (reference HREC/16/RCHM/84) and the Northern A Health and Disability Ethics Committee, New Zealand (reference 16/NTA/146). Hospitals agreeing to take part will obtain local research governance review. This includes a departmental agreement signed by both the clinical director of ED and inpatients and a data transfer agreement.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
