

Epithelial origin of eosinophilic esophagitis
- PMID: 29980278
- PMCID: PMC8034427
- DOI: 10.1016/j.jaci.2018.05.008
Epithelial origin of eosinophilic esophagitis
Abstract
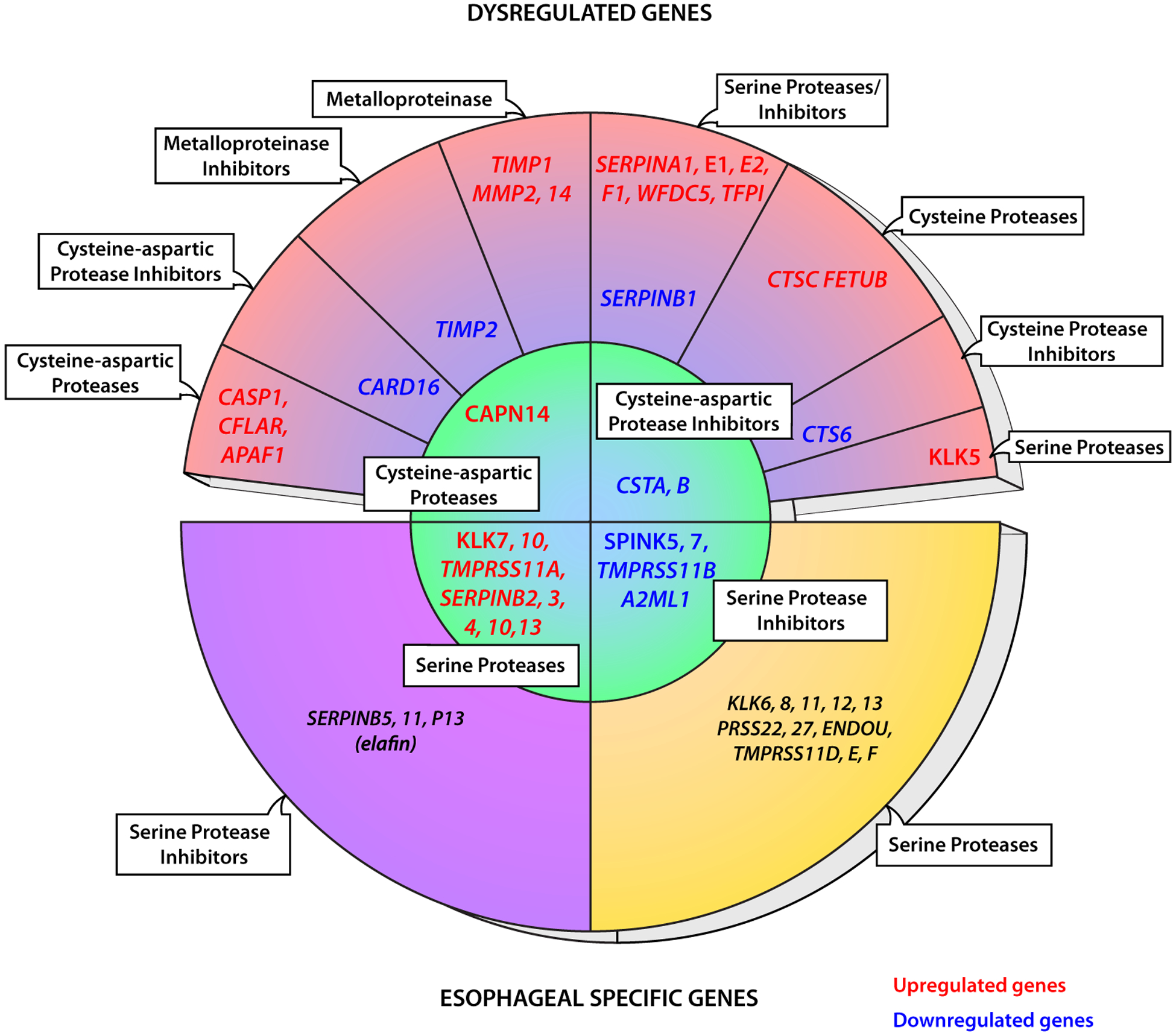
Eosinophilic esophagitis (EoE) is a chronic, allergen-driven inflammatory disease of the esophagus characterized predominantly by eosinophilic inflammation, leading to esophageal dysfunction. Converging data have placed the esophageal epithelium at the center of disease pathogenesis. In particular, the main EoE disease susceptibility loci at 2p23 and 5p22 encode for gene products that are produced by the esophageal epithelium: the intracellular protease calpain 14 and thymic stromal lymphopoietin, respectively. Furthermore, genetic and functional data establish a primary role for impaired epithelial barrier function in disease susceptibility and pathoetiology. Additionally, the EoE transcriptome, a set of genes dysregulated in the esophagi of patients with EoE, is enriched in genes that encode for proteins involved in esophageal epithelial cell differentiation. This transcriptome has a high proportion of esophagus-specific epithelial genes that are notable for the unexpected enrichment in genes encoding for proteases and protease inhibitors, as well as in IL-1 family genes, demonstrating a previously unappreciated role for innate immunity responses in the esophagus under homeostatic conditions. Among these pathways, basal production of the serine protease inhibitor, Kazal-type 7 (SPINK7) has been demonstrated to be part of the normal differentiation program of esophageal epithelium. Profound lost expression of SPINK7 occurs in patients with EoE and is sufficient for unleashing increased proteolytic activity (including urokinase plasminogen activator), impaired barrier function, and production of large quantities of proinflammatory and proallergic cytokines, including thymic stromal lymphopoietin. Collectively, we put forth a model in which the esophagus is normally equipped as an anti-inflammatory sensing organ and that defects in this pathway, mediated by epithelial protease/protease inhibitor imbalances, unleash inflammatory responses resulting in disorders, such as EoE.
Keywords: Eosinophilic esophagitis; Kazal type; eosinophilic oesophagitis; epithelial barrier; epithelial differentiation; esophageal epithelium; protease inhibitors; proteases; serine protease inhibitors.
Copyright © 2018. Published by Elsevier Inc.
Conflict of interest statement
Disclosure of potential conflict of interest: M. E. Rothenberg is a consultant for PulmOne, Spoon Guru, ClostraBio, Celgene, Shire, AstraZeneca, GlaxoSmithKline, Allakos, Adare, Regeneron, and Novartis; has an equity interest in the first 4 listed companies and Immune Pharmaceuticals; and has received royalties from reslizumab (Teva Pharmaceuticals) and UpToDate. M. Rochman, N. P. Azouz, and M. E. Rothenberg are inventors of patents owned by Cincinnati Children’s Hospital Medical Center.
Figures




References
-
- Abonia JP, Rothenberg ME. Eosinophilic esophagitis: rapidly advancing insights. Annu Rev Med 2012;63:421–34. - PubMed
-
- Noel RJ, Putnam PE, Rothenberg ME. Eosinophilic esophagitis. N Engl J Med 2004;351:940–1. - PubMed
-
- Safroneeva E, Coslovsky M, Kuehni CE, Zwahlen M, Haas NA, Panczak R, et al. Eosinophilic oesophagitis: relationship of quality of life with clinical, endoscopic and histological activity. Aliment Pharmacol Ther 2015;42:1000–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
