

Slow Potential at the Entrance of the Slow Conduction Zone in the Reentry Circuit of a Verapamil-Sensitive Atrial Tachycardia Originating From the Atrioventricular Annulus
- PMID: 29980519
- PMCID: PMC6064849
- DOI: 10.1161/JAHA.118.009223
Slow Potential at the Entrance of the Slow Conduction Zone in the Reentry Circuit of a Verapamil-Sensitive Atrial Tachycardia Originating From the Atrioventricular Annulus
Abstract
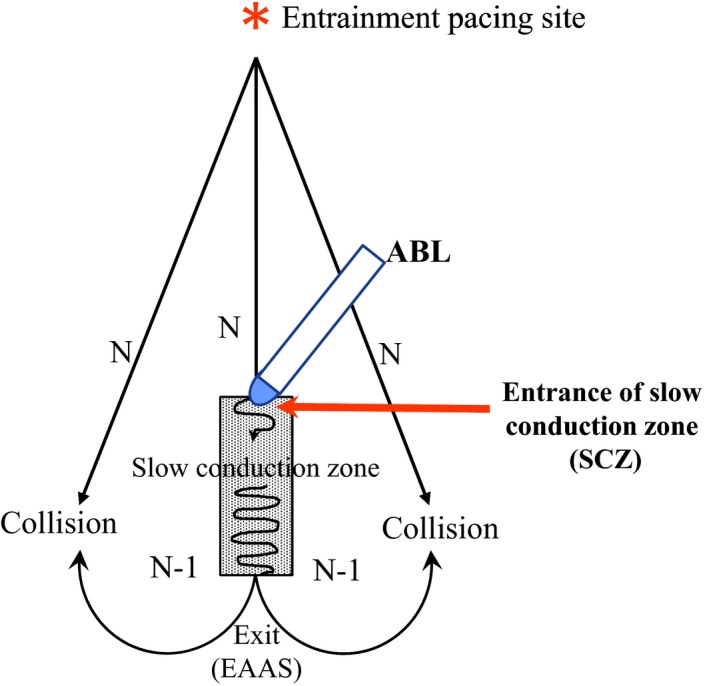
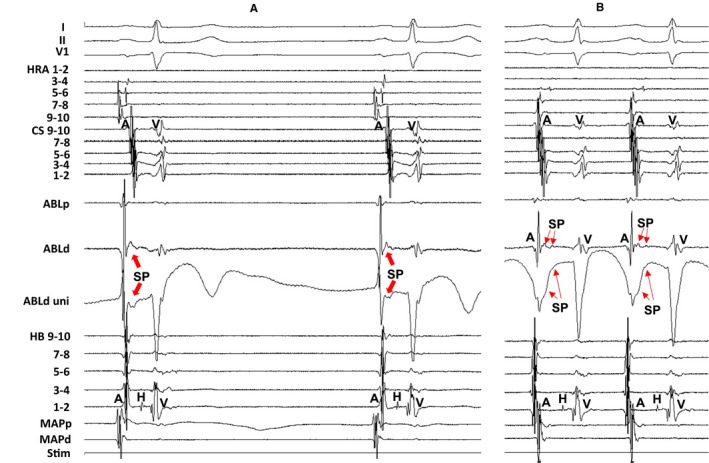
Background: Slow conduction zone in a verapamil-sensitive reentrant atrial tachycardia originating from atrioventricular annulus is composed of calcium channel-dependent tissue. We examined whether there was a slow potential (SP) at the entrance of the slow conduction zone.
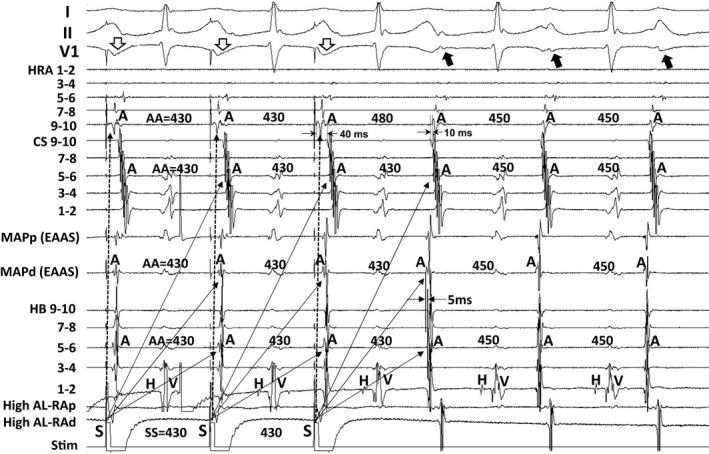
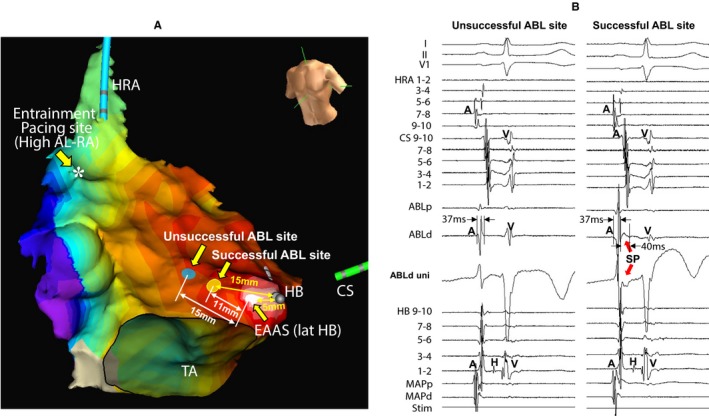
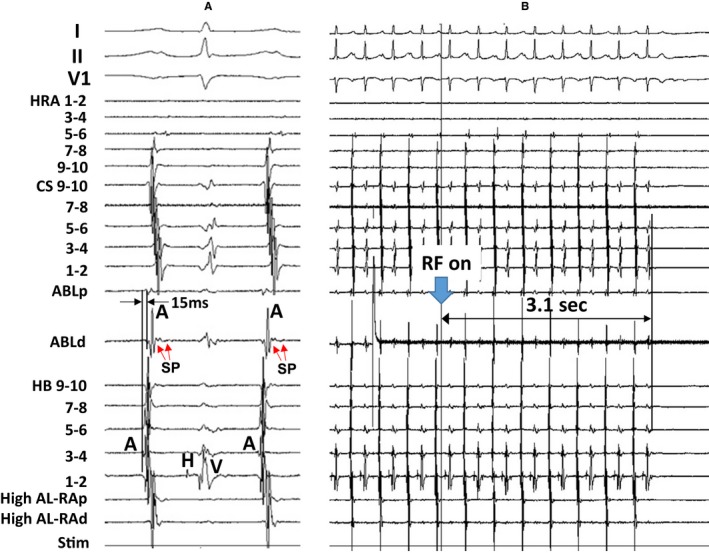
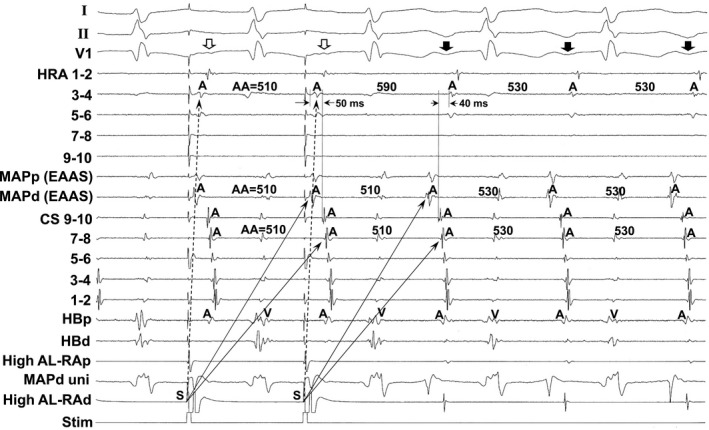
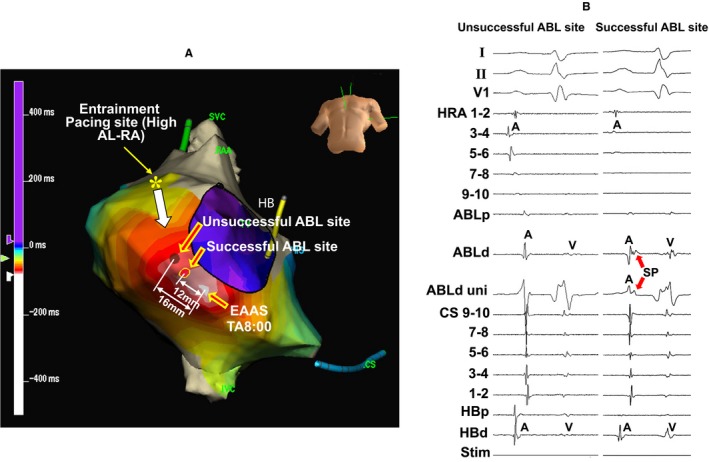
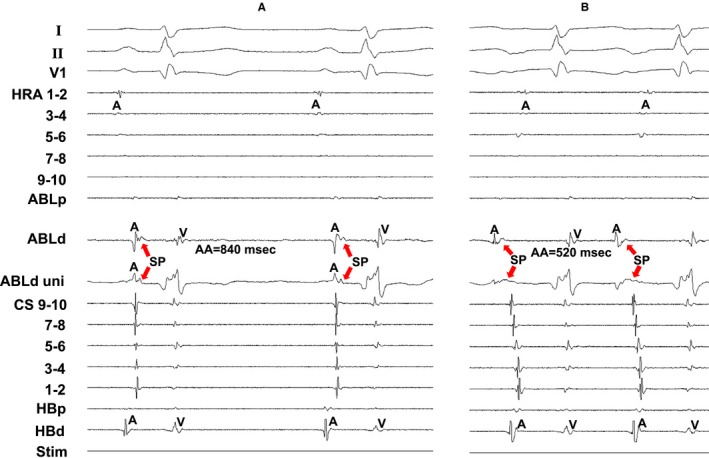
Methods and results: We first identified the pacing site from where manifest entrainment and orthodromic capture of the earliest atrial activation site were demonstrated in 40 atrioventricular annulus patients with atrioventricular annulus. Radiofrequency energy was then delivered 2 cm proximal to the earliest atrial activation site in the direction of entrainment pacing site and gradually advanced toward the earliest atrial activation site until atrial tachycardia termination to localize the entrance of the slow conduction zone. Electrogram characteristics were analyzed at successful and unsuccessful ablation sites. During sinus rhythm, SP was observed at all 40 successful sites, but was observed at only 12 unsuccessful sites (P<0.0001). During sinus rhythm, there was no significant difference in electrogram amplitude nor width of atrial electrogram between successful and unsuccessful sites (0.407±0.281 versus 0.487±0.447 mV [P=0.1989] and 37.0±9.2 versus 38.9±8.0 ms [P=0.1773]); however, SP amplitude and width at successful sites were significantly greater than those at unsuccessful sites (0.110±0.049 versus 0.025±0.046 mV [P<0.0001] and 38.8±13.4 versus 8.1±13.2 ms [P<0.0001]). During atrial tachycardia, SP amplitude was significantly attenuated (0.088±0.042 versus 0.110±0.049 mV, P<0.001) and SP width was significantly prolonged (47.8±14.1 versus 38.8±13.4 ms, P<0.0001) at successful sites.
Conclusions: SP was observed during sinus rhythm at the entrance of the slow conduction zone; however, SP amplitude was attenuated and SP width was prolonged during atrial tachycardia, suggesting that SP reflects the characteristics of calcium channel-dependent tissue involved in atrioventricular annulus reentry circuit.
Keywords: atrial tachycardia; catheter ablation; mapping.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
Demonstration of the Anatomical Tachycardia Circuit in Sinoatrial Node Reentrant Tachycardia: Analysis Using the Entrainment Method.J Am Heart Assoc. 2020 Jan 21;9(2):e014472. doi: 10.1161/JAHA.119.014472. Epub 2020 Jan 11. J Am Heart Assoc. 2020. PMID: 31928174 Free PMC article.
-
Demonstration of anatomic reentrant circuit in verapamil-sensitive atrial tachycardia originating from the atrioventricular annulus other than the vicinity of the atrioventricular node.Am J Cardiol. 2014 Jun 1;113(11):1822-8. doi: 10.1016/j.amjcard.2014.03.011. Epub 2014 Mar 15. Am J Cardiol. 2014. PMID: 24837259
-
Demonstration of anatomical reentrant tachycardia circuit in verapamil-sensitive atrial tachycardia originating from the vicinity of the atrioventricular node.Heart Rhythm. 2012 Sep;9(9):1475-83. doi: 10.1016/j.hrthm.2012.05.012. Epub 2012 May 11. Heart Rhythm. 2012. PMID: 22583842
-
Localization of the origin of the atrioventricular junctional rhythm induced during selective ablation of slow-pathway conduction in patients with atrioventricular node reentrant tachycardia.Am Heart J. 1996 May;131(5):937-46. doi: 10.1016/s0002-8703(96)90176-3. Am Heart J. 1996. PMID: 8615313 Review.
-
Electrophysiology of the A-V node in relation to A-V nodal reentry.Jpn Heart J. 1996 Sep;37(5):785-91. doi: 10.1536/ihj.37.785. Jpn Heart J. 1996. PMID: 8973390 Review.
Cited by
-
Demonstration of the Anatomical Tachycardia Circuit in Sinoatrial Node Reentrant Tachycardia: Analysis Using the Entrainment Method.J Am Heart Assoc. 2020 Jan 21;9(2):e014472. doi: 10.1161/JAHA.119.014472. Epub 2020 Jan 11. J Am Heart Assoc. 2020. PMID: 31928174 Free PMC article.
-
Outcomes of deep sedation for catheter ablation of paroxysmal supraventricular tachycardia, with adaptive servo ventilation.J Arrhythm. 2020 Dec 5;37(1):33-42. doi: 10.1002/joa3.12476. eCollection 2021 Feb. J Arrhythm. 2020. PMID: 33664884 Free PMC article.
-
Atrioventricular Ring Tachycardias: Atypical Fast-Slow Atrioventricular Nodal Reentrant Tachycardia and Atrial Tachycardia Share a Common Arrhythmogenic Substrate-A Unifying Proposal.Rev Cardiovasc Med. 2022 Oct 28;23(11):369. doi: 10.31083/j.rcm2311369. eCollection 2022 Nov. Rev Cardiovasc Med. 2022. PMID: 39076194 Free PMC article. Review.
-
Target potential for ablation in adenosine-sensitive atrial tachycardia originating from the vicinity of the atrioventricular node identified by the LUMIPOINT software.HeartRhythm Case Rep. 2023 Dec 15;10(3):203-207. doi: 10.1016/j.hrcr.2023.12.009. eCollection 2024 Mar. HeartRhythm Case Rep. 2023. PMID: 38496741 Free PMC article. No abstract available.
-
Ripple map delineation of the reentrant circuit in a tricuspid annular atrial tachycardia mimicking focal activity.Indian Pacing Electrophysiol J. 2024 Jul-Aug;24(4):229-232. doi: 10.1016/j.ipej.2024.06.004. Epub 2024 Jun 18. Indian Pacing Electrophysiol J. 2024. PMID: 38901653 Free PMC article.
References
-
- Haissaguerre M, Gaito F, Fischer B, Commenges D, Montserrat P, d'Ivernois C, Lemetayer P, Warin JF. Elimination of atrioventricular nodal reentrant tachycardia using discrete slow potentials to guide application of radiofrequency energy. Circulation. 1992;85:2162–2175. - PubMed
-
- de Bakker JM, Coronel R, McGuire MA, Vermeulen JT, Opthof T, Tasseron S, van Hemel NM, Defauw JJ. Slow potentials in the atrioventricular junctional area of patients operated on for atrioventricular node tachycardias and in isolated porcine hearts. J Am Coll Cardiol. 1994;23:709–715. - PubMed
-
- Yamabe H, Okumura K, Tsuchiya T, Tabuchi T, Iwasa A, Yasue H. Slow potential‐guided radiofrequency catheter ablation in atrioventricular nodal reentrant tachycardia: characteristics of the potential associated with successful ablation. Pacing Clin Electrophysiol. 1998;21:2631–2640. - PubMed
-
- Iesaka Y, Takahashi A, Goya M, Soejima Y, Okamoto Y, Fujiwara H, Aonuma K, Nogami A, Hiroe M, Marumo F, Hiraoka M. Adenosine‐sensitive atrial reentrant tachycardia originating from the atrioventricular nodal transitional area. J Cardiovasc Electrophysiol. 1997;8:854–864. - PubMed
-
- Yamabe H, Tanaka Y, Okumura K, Morikami Y, Kimura Y, Hokamura Y, Ogawa H. Electrophysiologic characteristics of verapamil‐sensitive atrial tachycardia originating from the atrioventricular annulus. Am J Cardiol. 2005;95:1425–1430. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
