

The effect of socio-demographic factors on mental health and addiction high-cost use: a retrospective, population-based study in Saskatchewan
- PMID: 29981109
- PMCID: PMC6267642
- DOI: 10.17269/s41997-018-0101-2
The effect of socio-demographic factors on mental health and addiction high-cost use: a retrospective, population-based study in Saskatchewan
Abstract
Objective: A small proportion of the population accounts for the majority of healthcare costs. Mental health and addiction (MHA) patients are consistently high-cost. We aimed to delineate factors amenable to public health action that may reduce high-cost use among a cohort of MHA clients in Saskatoon, Saskatchewan.
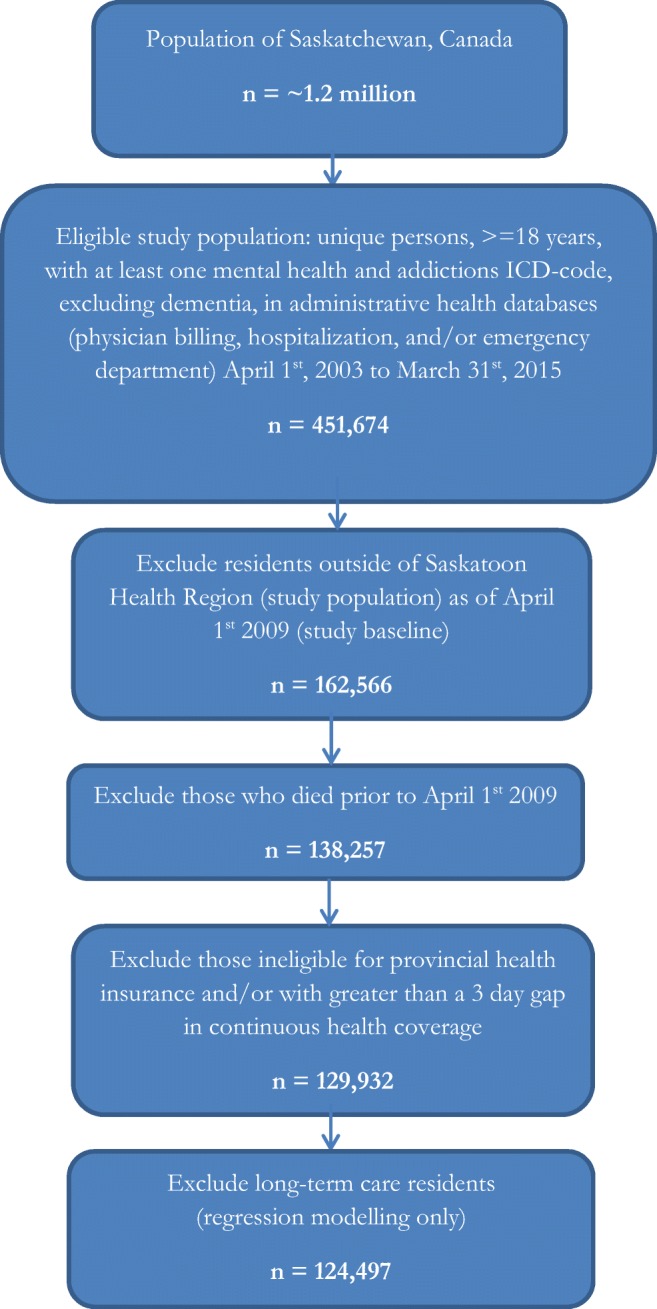
Methods: We conducted a population-based retrospective cohort study. Administrative health data from fiscal years (FY) 2009-2015, linked at the individual level, were analyzed (n = 129,932). The outcome of interest was ≥ 90th percentile of costs for each year under study ('persistent high-cost use'). Descriptive analyses were followed by logistic regression modelling; the latter excluded long-term care residents.
Results: The average healthcare cost among study cohort members in FY 2009 was ~ $2300; for high-cost users it was ~ $19,000. Individuals with unstable housing and hospitalization(s) had increased risk of persistent high-cost use; both of these effects were more pronounced as comorbidities increased. Patients with schizophrenia, particularly those under 50 years old, had increased probability of persistent high-cost use. The probability of persistent high-cost use decreased with good connection to a primary care provider; this effect was more pronounced as the number of mental health conditions increased.
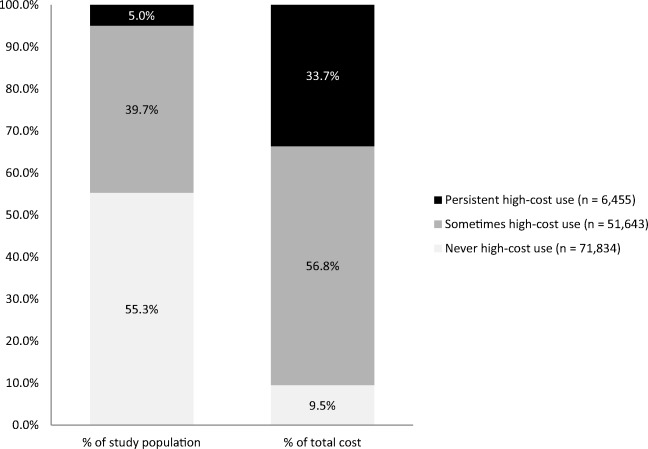
Conclusion: Despite constituting only 5% of the study cohort, persistent high-cost MHA clients (n = 6455) accounted for ~ 35% of total costs. Efforts to reduce high-cost use should focus on reduction of multimorbidity, connection to a primary care provider (particularly for those with more than one MHA), young patients with schizophrenia, and adequately addressing housing stability.
Objectif: Une faible proportion de la population compte pour la majorité des coûts des soins de santé. Les patients en santé mentale et en toxicomanie (SMT) engendrent systématiquement des coûts élevés. Nous avons cherché à délimiter les facteurs qui se prêteraient à des mesures de santé publique susceptibles de réduire l’utilisation à coût élevé dans une cohorte d’usagers en SMT de Saskatoon (Saskatchewan).
Méthode: Nous avons mené une étude de cohorte populationnelle rétrospective. Les données administratives sur la santé des exercices 2009 à 2015, jumelées au niveau individuel, ont été analysées (n = 129 932). Le résultat qui nous intéressait était ≥ au 90e centile des coûts pour chaque exercice à l’étude (« utilisation à coût élevé persistante »). Des analyses descriptives ont été suivies par des modèles de régression logistique; ces derniers ont exclu les résidents en soins de longue durée.
Résultats: Le coût moyen des soins de santé chez les membres de la cohorte étudiée était d’environ 2300 $ durant l’exercice 2009; pour les utilisateurs à coût élevé, il était d’environ 19 000 $. Les personnes vivant dans des conditions de logement précaires et ayant été hospitalisées une ou plusieurs fois présentaient un risque accru d’utilisation à coût élevé persistante; les deux effets s’accentuaient avec la présence de comorbidités. Les patients schizophrènes, surtout ceux de moins de 50 ans, présentaient une probabilité accrue d’utilisation à coût élevé persistante. La probabilité d’utilisation à coût élevé persistante diminuait avec la qualité du lien vers un dispensateur de soins primaires; cet effet s’accentuait avec l’augmentation du nombre de troubles de santé mentale.
Conclusion: Bien qu’ils n’aient constitué que 5 % de la cohorte à l’étude, les usagers en SMT faisant une utilisation à coût élevé persistante des soins de santé (n = 6455) comptaient pour ~ 35 % des coûts totaux. Les efforts pour réduire l’utilisation à coût élevé devraient se concentrer sur la réduction des comorbidités, sur le lien vers un dispensateur de soins primaires (surtout pour les patients présentant plus d’un problème de SMT) et sur les jeunes patients schizophrènes, et ils devraient suffisamment tenir compte de la précarité du logement.
Keywords: High-cost users; Mental health and addictions; Social determinants of health.
Conflict of interest statement
The authors declare that they have no conflict of interest. This study is based in part on de-identified data provided by the Saskatchewan Ministry of Health and eHealth Saskatchewan. The interpretation and conclusions contained herein do not necessarily represent those of the Government of Saskatchewan, the Saskatchewan Ministry of Health, or eHealth Saskatchewan. Data used in this report were also made available by the Saskatoon Regional Health Authority. Any opinions expressed by the authors do not necessarily reflect the opinion of the Saskatoon Regional Health Authority.
Figures
References
-
- Canadian Institute for Health Information. (2008). Physicians in Canada: the status of alternative payment programs, 2005–2006. Retrieved May 2, 2018, from http://publications.gc.ca/collections/collection_2008/cihi-icis/H115-13-...
-
- Canadian Institute for Health Information (CIHI). (2015a). MIS Standards Retrieved January 20, 2016, from https://www.cihi.ca/en/data-and-standards/standards/mis-standards
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
