

Registration and publication of emergency and elective randomised controlled trials in surgery: a cohort study from trial registries
- PMID: 29982216
- PMCID: PMC6042627
- DOI: 10.1136/bmjopen-2018-021700
Registration and publication of emergency and elective randomised controlled trials in surgery: a cohort study from trial registries
Abstract
Objectives: Emergency surgical practice constitutes 50% of the workload for surgeons, but there is a lack of high quality randomised controlled trials (RCTs) in emergency surgery. This study aims to establish the differences between the registration, completion and publication of emergency and elective surgical trials.
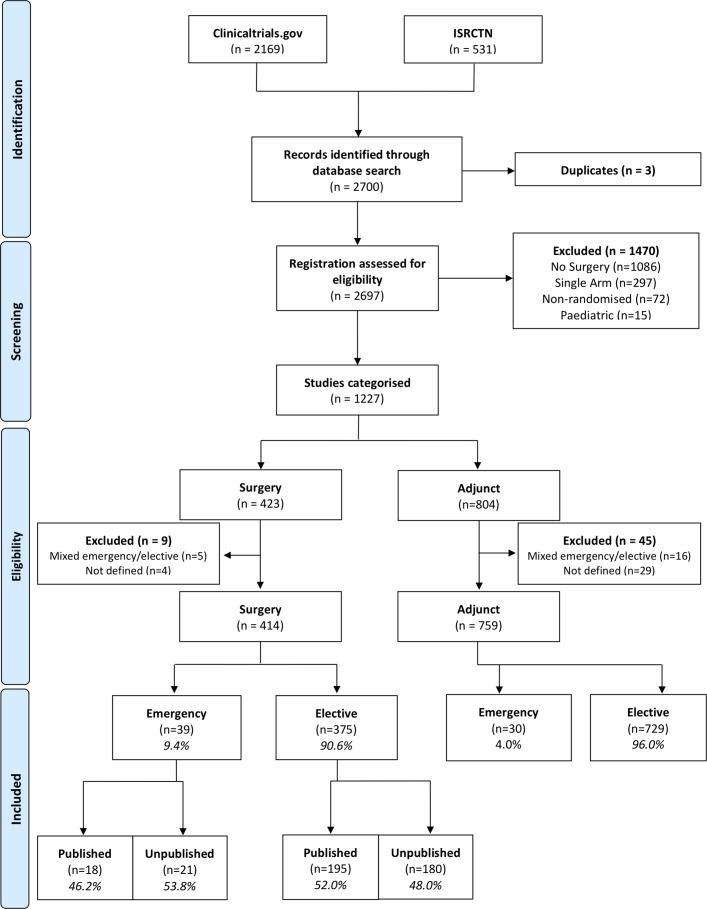
Design: The clinicaltrials.gov and ISRCTN.com trials registry databases were searched for RCTs between 12 July 2010 and 12 July 2012 using the keyword 'surgery'. Publications were systematically searched for in Pubmed, MEDLINE and EMBASE.
Participants: Results with no surgical interventions were excluded. The remaining results were manually categorised into 'emergency' or 'elective' and 'surgical' or 'adjunct' by two reviewers.
Primary outcome measures: Number of RCTs registered in emergency versus elective surgery.
Secondary outcome measures: Number of RCTs published in emergency versus elective surgery; reasons why trials remain unpublished; funding, sponsorship and impact of published articles; number of adjunct trials registered in emergency and elective surgery.
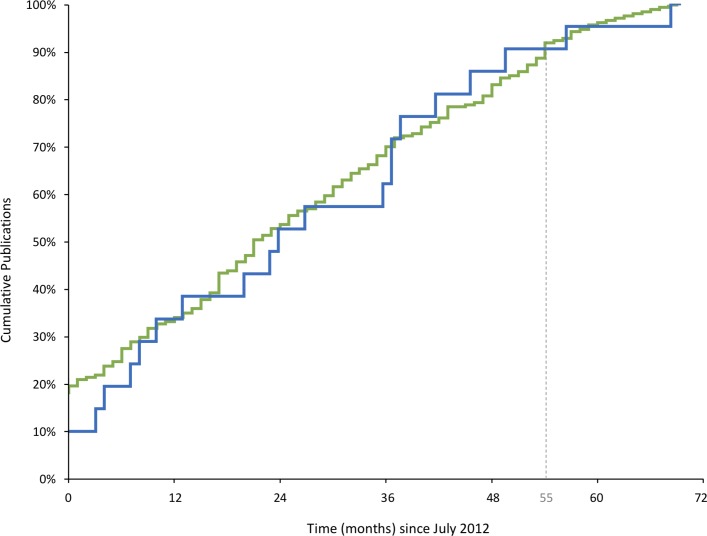
Results: 2700 randomised trials were registered. 1173 trials were on a surgical population and of these, 414 trials were studying surgery. Only 9.4% (39/414) of surgical trials were in emergency surgery. The proportion of trials successfully published did not significantly differ between emergency and elective surgery (0.46 vs 0.52; mean difference (MD) -0.06, 95% CI -0.24 to 0.12). Unpublished emergency surgical trials were statistically equally likely to be terminated early compared with elective trials (0.33 vs 0.16; MD -0.18, 95% CI -0.06 to 0.41). Low accrual accounted for a similar majority in both groups (0.43 vs 0.46; MD -0.04, 95% CI -0.48 to 0.41). Unpublished trials in both groups were statistically equally likely to still be planning publication (0.52 vs 0.71; MD -0.18, 95% CI -0.43 to 0.07).
Conclusion: Fewer RCTs are registered in emergency than elective surgery. Once trials are registered both groups are equally likely to be published.
Keywords: emergency; surgery.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- RCSEng. Emergency Surgery - Standards for unscheduled surgical care, 2011. https://www.google.co.uk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=3&cad=rj... (5 Oct 2017).
-
- McCord C, Ozgediz D, Beard JH, et al. General Surgical Emergencies. Essential Surgery: Disease Control Priorities 2015. http://www.ncbi.nlm.nih.gov/pubmed/26741004 (3 Jul 2017).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources