

Safety and efficacy of depatuxizumab mafodotin + temozolomide in patients with EGFR-amplified, recurrent glioblastoma: results from an international phase I multicenter trial
- PMID: 29982805
- PMCID: PMC6303422
- DOI: 10.1093/neuonc/noy091
Safety and efficacy of depatuxizumab mafodotin + temozolomide in patients with EGFR-amplified, recurrent glioblastoma: results from an international phase I multicenter trial
Abstract
Background: Patients with glioblastoma (GBM) have a dismal prognosis. Nearly all will relapse with no clear standard of care for recurrent disease (rGBM). Approximately 50% of patients have tumors harboring epidermal growth factor receptor (EGFR) amplification. The antibody-drug conjugate depatuxizumab mafodotin (depatux-m) binds cells with EGFR amplification, is internalized, and releases a microtubule toxin, killing the cell. Here we report efficacy, safety and pharmacokinetics (PK) of depatux-m + temozolomide (TMZ) in patients with EGFR-amplified rGBM.
Methods: M12-356 (NCT01800695) was an open-label study encompassing patients with newly diagnosed or rGBM across 3 treatment arms. Results are reported for adults with EGFR-amplified, measurable rGBM who received depatux-m (0.5-1.5 mg/kg) on days 1 and 15, and TMZ (150-200 mg/m2) on days 1-5 in a 28-day cycle. Patients were bevacizumab and nitrosourea naïve.
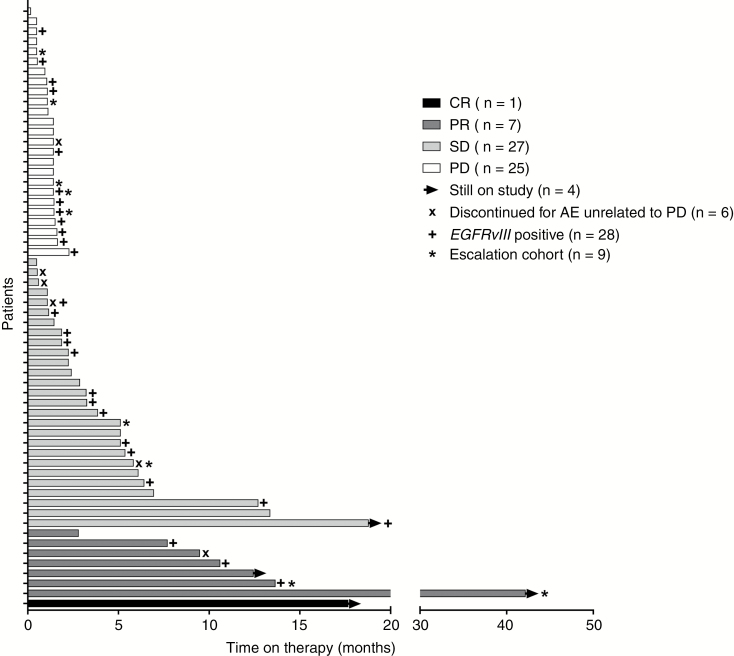
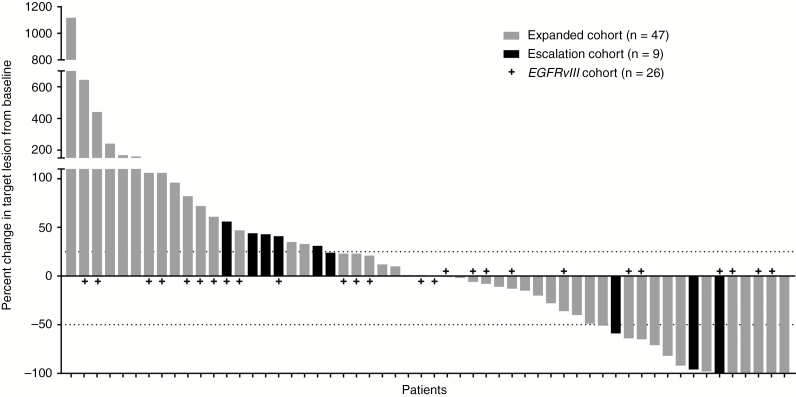
Results: There were 60 patients, median age 56 years (range, 20-79). Fifty-nine patients previously received TMZ. Common adverse events (AEs) were blurred vision (63%), fatigue (38%), and photophobia (35%). Grades 3/4 AEs were split between ocular and non-ocular AEs, occurring in 22% of patients each. Systemic PK exposure of depatux-m was dose proportional. The objective response rate was 14.3%, the 6-month progression-free survival rate was 25.2%, and the 6-month overall survival rate was 69.1%.
Conclusions: Depatux-m + TMZ displayed an AE profile similar to what was described previously. Antitumor activity in this TMZ-refractory population was encouraging. Continued study of depatux-m in patients with EGFR-amplified, newly diagnosed, or recurrent GBM is ongoing in 2 global, randomized trials (NCT02573324, NCT02343406).
Figures
References
-
- Stupp R, Hegi ME, Mason WP, et al. ; European Organisation for Research and Treatment of Cancer Brain Tumour and Radiation Oncology Groups; National Cancer Institute of Canada Clinical Trials Group Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(5):459–466. - PubMed
-
- Chinot OL, Wick W, Mason W, et al. Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N Engl J Med. 2014;370(8):709–722. - PubMed
-
- Franceschi E, Minichillo S, Brandes AA. Pharmacotherapy of glioblastoma: established treatments and emerging concepts. CNS Drugs. 2017;31(8):675–684. - PubMed
-
- Taal W, Oosterkamp HM, Walenkamp AM, et al. Single-agent bevacizumab or lomustine versus a combination of bevacizumab plus lomustine in patients with recurrent glioblastoma (BELOB trial): a randomised controlled phase 2 trial. Lancet Oncol. 2014;15(9):943–953. - PubMed
-
- Seystahl K, Wick W, Weller M. Therapeutic options in recurrent glioblastoma—an update. Crit Rev Oncol Hematol. 2016;99:389–408. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
