

Health inequities and cancer survival in Manizales, Colombia: a population-based study
- PMID: 29983465
- PMCID: PMC6018827
- DOI: 10.25100/cm.v49i1.3629
Health inequities and cancer survival in Manizales, Colombia: a population-based study
Abstract
Objective: To analyze differences in survival of breast, cervical, lung, prostate and stomach cancer by health insurance regime (HIR) and socioeconomic position (SEP) in an intermediate city in a middle-income country.
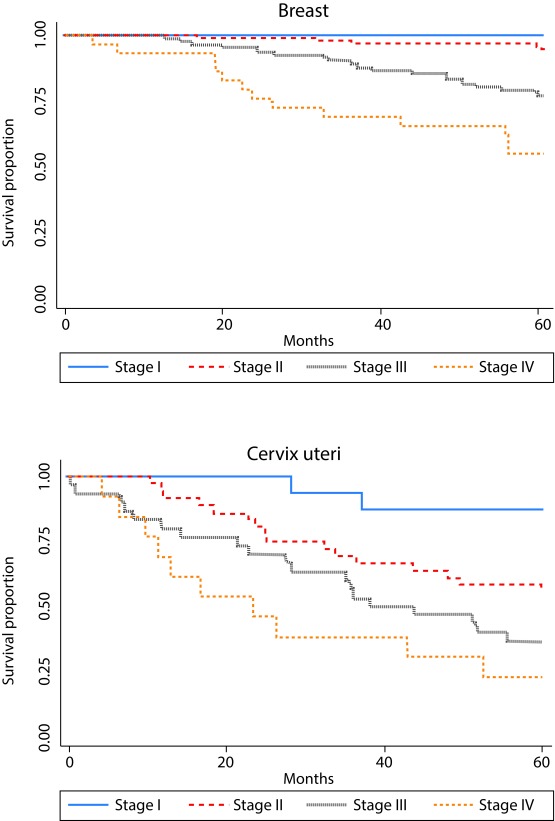
Methods: All patients with breast, cervix uteri, lung, prostate and stomach cancer diagnosed between 2003 and 2007 and characterized by the Manizales population-based Cancer Registry (MCR) were included and followed up to a maximum of 5 years for identifying deaths. Survival probabilities estimated by HIR were defined according to the type of affiliation at the date of diagnosis, and by socioeconomic stratification of residence (SS) as indicator of SEP, stratifying for other prognostic factors using Kaplan-Meier methods. Cox proportional hazard models were fitted for multivariate analysis.
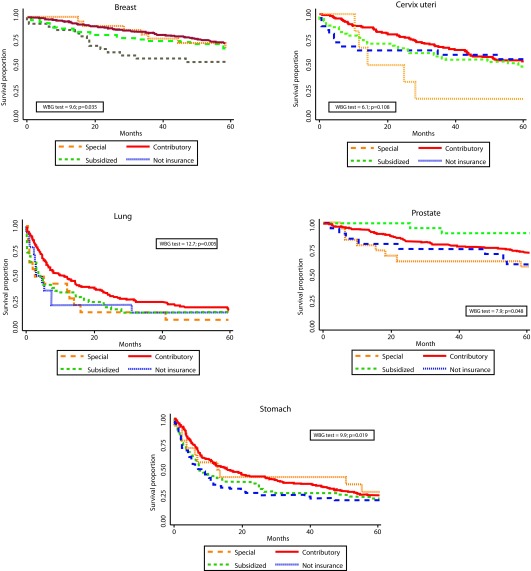
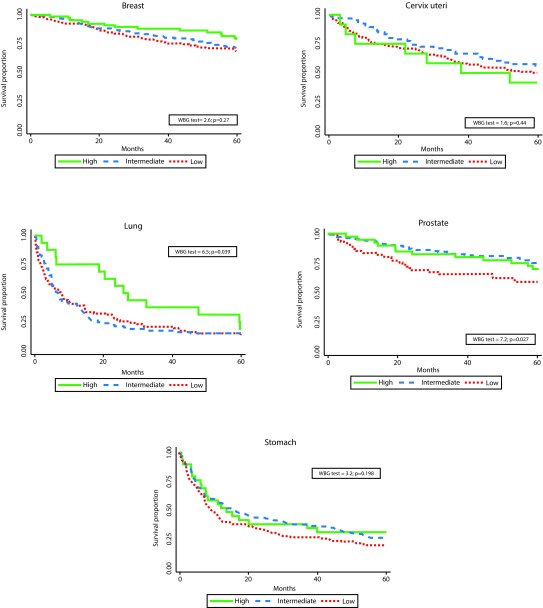
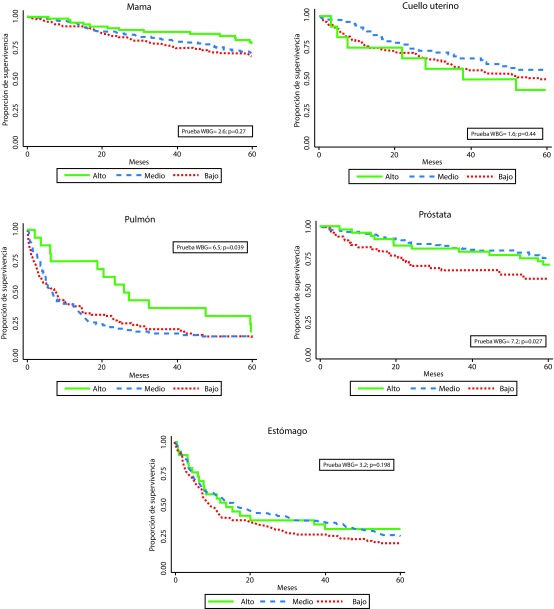
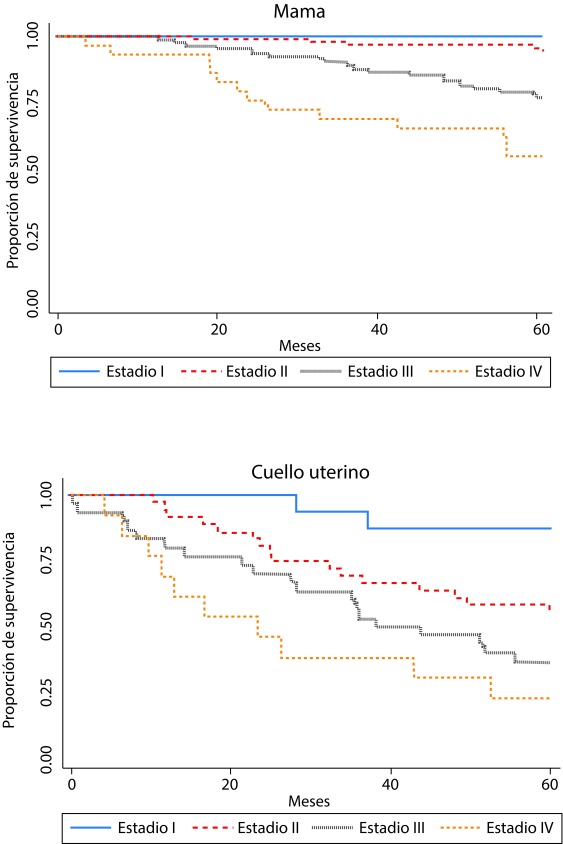
Results: A total of 1,384 cases and 700 deaths were analyzed. Five-year observed survival was 71.0% (95% IC: 66.1-75.3) for breast, 51.4% (95% IC: 44.6-57.9) for cervix, 15.4% (95% IC: 10.7-20.8) for lung, 71.1% (95% IC: 65.3-76.1) for prostate and 23.8% (95% IC: 19.3-28.6) for stomach. Statistically significant differences in survival by HIR were observed for breast, lung, prostate, and stomach - with poorer survival for the subsidized and uninsured patients. Differences by SS were observed for lung and prostate. Differences in survival by HIR were independent of SS, and viceversa.
Conclusions: Important inequities in cancer survival exist related to HIR and SEP. Possible explanations include underlying comorbidities, late stage at diagnosis, or barriers to timely and effective treatment.
Objetivo: Analizar la supervivencia de pacientes con cáncer de mama, cuello uterino, pulmón, próstata y estómago según régimen de aseguramiento en salud (RAS) y posición socioeconómica (PSE) en una ciudad intermedia de un país de medianos ingresos.
Métodos: Se incluyeron todos los pacientes con cáncer de mama, cuello uterino, pulmón, próstata y estómago diagnosticados entre 2003 y 2007 y caracterizados por el Registro Poblacional de Cáncer de Manizales, quienes fueron seguidos hasta un máximo de cinco años para identificar los fallecimientos. Las probabilidades de supervivencia estimada según RAS fueron definidas de acuerdo con el tipo de afiliación al momento del diagnóstico, y según el estrato socioeconómico de la residencia como indicador de PSE, estratificando por otros factores pronósticos y utilizando el método de Kaplan-Meier. Para el análisis multivariado se ajustaron modelos de riesgos proporcionales de Cox.
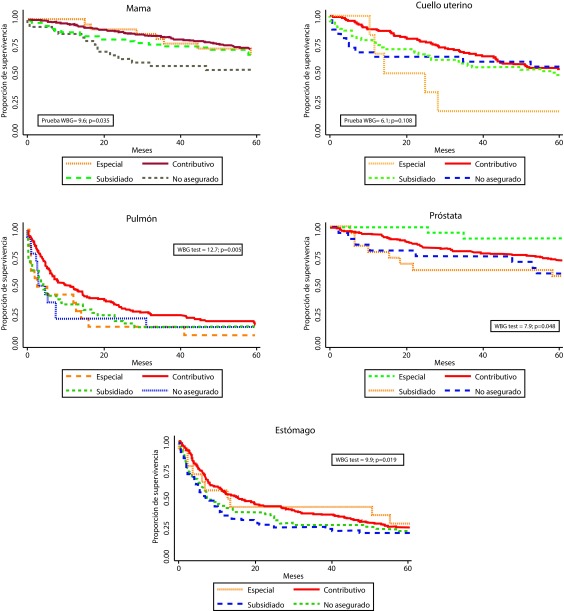
Resultados: Se analizaron en total 1.384 casos y 700 muertes. La supervivencia observada a cinco años fue 71.0% (IC 95%: 66.1-75.3) para cáncer de mama, 51.4% (44.6-57.9) para cuello uterino, 15.4% (10.7-20.8) para pulmón, 71.1% (65.3-76.1) para próstata, y 23.8% (19.3-28.6) para estómago. Se observaron diferencias estadísticamente significativas en la supervivencia según RAS para mama, pulmón, próstata y estómago, con supervivencia más pobre en los pacientes del régimen subsidiado y no asegurados. Se observaron diferencias por estrato socioeconómico en los cánceres de pulmón y próstata. Las diferencias por RAS fueron independientes del estrato socioeconómico y viceversa.
Conclusiones: Existen importantes inequidades en la supervivencia de pacientes con cáncer relacionadas con el RAS y con la PSE. Las posibles explicaciones incluyen comorbilidades subyacentes, diagnóstico tardío y barreras para el acceso al tratamiento oportuno y efectivo.
Keywords: insurance, health; malignant neoplasms; socioeconomic factors; survival analysis.
Conflict of interest statement
Conflict of interest: None of the authors have any conflicts of interest to be reported. The funding had no influence in study design; in the collection, analysis and interpretation of data; in the writing of the report; neither in the decision to submit the article for publication.
Figures
References
-
- Woods L, Rachet P, Coleman M. Origins of socio-economic inequalities in cancer survival a review. Ann Oncol. 2006;17(1):5–19. - PubMed
-
- Booth CM, Li G, Zhang-Salomons J, Mackillop WJ. The impact of socioeconomic status on stage of cancer at diagnosis and survival A population-based study in Ontario, Canada. Cancer. 2010;116(17):4160–4167. - PubMed
-
- Eaker S, Halmin M, Bellocco R, Bergkvist L, Ahlgren J, Holmberg L. Social differences in breast cancer survival in relation to patient management within a National Health Care System (Sweden) Int J Cancer. 2009;124(1):180–187. - PubMed
-
- Newmann SJ, Garner EO. Social inequities along the cervical cancer continuum A structured review. Cancer Causes Control. 2005;16(1):63–70. - PubMed
-
- Berglund A, Holmberg L, Tishelman C, Wagenius G, Eaker S, Lambe M. Social inequalities in non-small cell lung cancer management and survival a population-based study in central Sweden. Thorax. 2010;65(4):327–333. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
