

Prognostic impact of the number of lymph nodes examined in different stages of colorectal mucinous adenocarcinoma
- PMID: 29983574
- PMCID: PMC6026586
- DOI: 10.2147/OTT.S163076
Prognostic impact of the number of lymph nodes examined in different stages of colorectal mucinous adenocarcinoma
Abstract
Background: Mucinous adenocarcinoma (MC) is a special kind of colorectal adenocarcinoma that occurs more frequently in young patients and females, but the prognostic effect of lymph nodes in MC patients is unclear. This population-based study was conducted to analyze the prognostic value of the number of lymph nodes examined in different stages of colorectal MC.
Methods: We included 17,001 MC patients from the Surveillance, Epidemiology, and End Results program database between 2003 and 2013, of which 12,812 (75%) had >12 lymph nodes examined.
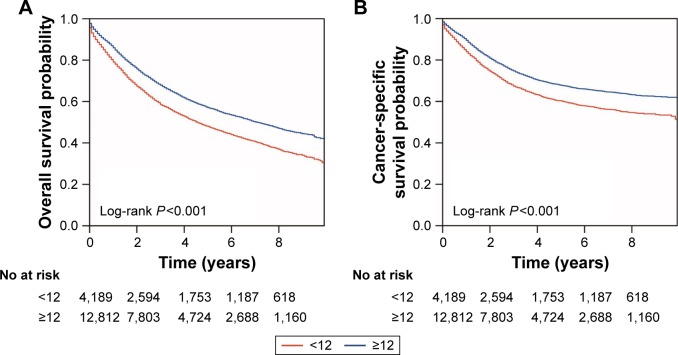
Results: Compared to the group with insufficient lymph nodes examined, patients with more lymph nodes (>12) examined tended to come from east and central America, were more frequently female and young, were diagnosed after 2008, had larger-sized tumors of less differentiated grade and in later stages, had not received radiation therapy and had more positive nodal status. Patients with more lymph nodes (>12) examined demonstrated significantly better survival than those with insufficient lymph nodes examined only in stages II and III (stage II: overall, P<0.001; cancer-specific, P<0.001; stage III: overall, P=0.093; cancer-specific, P=0.032), even though the overall (P<0.001) and cancer-specific survival (P<0.001) showed significant differences between the two groups. Both univariate (overall, HR=0.739, 95% CI=0.703-0.777, P<0.001; cancer-specific, HR=0.742, 95% CI=0.698-0.788, P<0.001) and multivariate (overall, HR=0.601, 95% CI=0.537-0.673, P<0.001; cancer-specific, HR=0.582, 95% CI=0.511-0.664, P<0.001) Cox proportional hazards models verified the association between >12 lymph nodes examined and better survival.
Conclusion: More number of lymph nodes (.12) examined significantly increased the survival probability of MC patients in stages II and III, but had no significant influence on patients in stages I and IV, indicating the effect of number of lymph nodes examined was a stage-dependent prognostic factor in clinical utility.
Keywords: mucinous carcinoma; number of lymph nodes examined; stages.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures


References
-
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–2917. - PubMed
-
- Simkens GA, van de Velde CJ, van Krieken JH, et al. Histological subtype and systemic metastases strongly influence treatment and survival in patients with synchronous colorectal peritoneal metastases. Eur J Surg Oncol. 2016;42:794–800. - PubMed
-
- Hermanek P. Colorectal carcinoma: histopathological diagnosis and staging. Baillieres Clin Gastroenterol. 1989;3:511–529. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
