

Infant and Young Child Feeding (IYCF) Practices Improved in 2 Districts in Nepal during the Scale-Up of an Integrated IYCF and Micronutrient Powder Program
- PMID: 29984348
- PMCID: PMC6022604
- DOI: 10.1093/cdn/nzy019
Infant and Young Child Feeding (IYCF) Practices Improved in 2 Districts in Nepal during the Scale-Up of an Integrated IYCF and Micronutrient Powder Program
Abstract
Background: Three-quarters of the ≥50 programs that use micronutrient powders (MNPs) integrate MNPs into infant and young child feeding (IYCF) programs, with limited research on impacts on IYCF practices.
Objective: This study assessed changes in IYCF practices in 2 districts in Nepal that were part of a post-pilot scale-up of an integrated IYCF-MNP program.
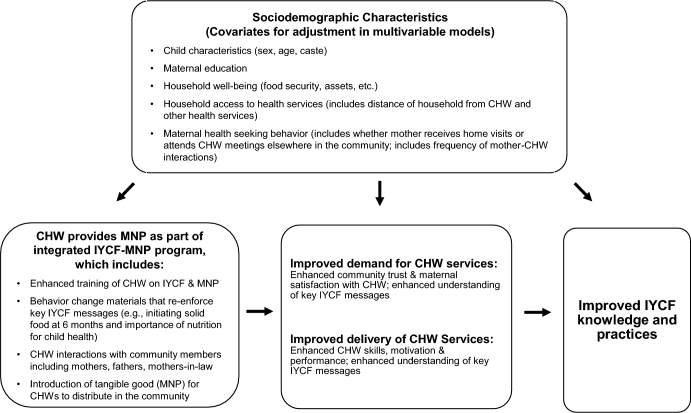
Methods: This analysis used cross-sectional surveys (n = 2543 and 2578 for baseline and endline) representative of children aged 6-23 mo and their mothers in 2 districts where an IYCF program added MNP distributions through female community health volunteers (FCHVs) and health workers (HWs). Multivariable log-binomial models estimated prevalence ratios comparing reported IYCF at endline with baseline and at endline on the basis of exposure to different sources of IYCF information. Mothers who received FCHV-IYCF counseling with infrequent (≤1 time/mo) and frequent (>1 time/mo) interactions were compared with mothers who never received FCHV-IYCF counseling. The receipt of HW-IYCF counseling and receipt of MNPs from an FCHV (both yes or no) were also compared.
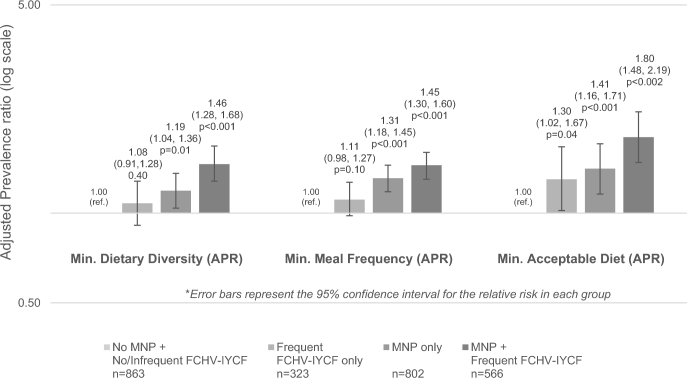
Results: The prevalence of minimum dietary diversity (MDD) and minimum acceptable diet (MAD) was significantly higher at endline than at baseline. In analyses from endline, compared with mothers who never received FCHV counseling, only mothers in the frequent FCHV-IYCF counseling group were more likely to report feeding the minimum meal frequency (MMF) and MAD, with no difference for the infrequent FCHV-IYCF counseling group in these indicators. HW-IYCF counseling was not associated with these indicators. Mothers who received MNPs from their FCHV were more likely to report initiating solid foods at 6 mo and feeding the child the MDD, MMF, and MAD compared with mothers who did not, adjusting for HW- and FCHV-IYCF counseling and demographic covariates.
Conclusions: Incorporating MNPs into the Nepal IYCF program did not harm IYCF and may have contributed to improvements in select practices. Research that uses experimental designs should verify whether integrated IYCF-MNP programs can improve IYCF practices.
Keywords: complementary feeding; dietary diversity; home-based fortification; infant and young child feeding; micronutrient powders; point-of-use fortification.
Figures
Similar articles
-
Predictors of micronutrient powder (MNP) knowledge, coverage, and consumption during the scale-up of an integrated infant and young child feeding (IYCF-MNP) programme in Nepal.Matern Child Nutr. 2019 Oct;15(S5):e12712. doi: 10.1111/mcn.12712. Matern Child Nutr. 2019. PMID: 31622040 Free PMC article.
-
Changes in growth, anaemia, and iron deficiency among children aged 6-23 months in two districts in Nepal that were part of the post-pilot scale-up of an integrated infant and young child feeding and micronutrient powder intervention.Matern Child Nutr. 2019 Apr;15(2):e12693. doi: 10.1111/mcn.12693. Epub 2018 Oct 12. Matern Child Nutr. 2019. PMID: 30226293 Free PMC article.
-
The Impact of Integrated Infant and Young Child Feeding and Micronutrient Powder Intervention on Feeding Practices and Anemia in Children Aged 6-23 Months in Madagascar.Nutrients. 2017 Jun 7;9(6):581. doi: 10.3390/nu9060581. Nutrients. 2017. PMID: 28590440 Free PMC article.
-
The potential role of micronutrient powders to improve complementary feeding practices.Matern Child Nutr. 2017 Oct;13 Suppl 2(Suppl 2):e12464. doi: 10.1111/mcn.12464. Matern Child Nutr. 2017. PMID: 29032625 Free PMC article. Review.
-
Home fortification of foods with multiple micronutrient powders for health and nutrition in children under two years of age.Cochrane Database Syst Rev. 2020 Feb 28;2(2):CD008959. doi: 10.1002/14651858.CD008959.pub3. Cochrane Database Syst Rev. 2020. PMID: 32107773 Free PMC article.
Cited by
-
Unintended consequences of programmatic changes to infant and young child feeding practices in Bangladesh.Matern Child Nutr. 2021 Apr;17(2):e13077. doi: 10.1111/mcn.13077. Epub 2020 Oct 16. Matern Child Nutr. 2021. PMID: 33063946 Free PMC article.
-
Predictors of micronutrient powder (MNP) knowledge, coverage, and consumption during the scale-up of an integrated infant and young child feeding (IYCF-MNP) programme in Nepal.Matern Child Nutr. 2019 Oct;15(S5):e12712. doi: 10.1111/mcn.12712. Matern Child Nutr. 2019. PMID: 31622040 Free PMC article.
-
An Integrated Enhanced Infant and Young Child Feeding (IYCF) and Micronutrient Powder Intervention Improved Select IYCF Practices Among Caregivers of Children Aged 12-23 Months in Eastern Uganda.Curr Dev Nutr. 2021 Jan 29;5(2):nzab003. doi: 10.1093/cdn/nzab003. eCollection 2021 Feb. Curr Dev Nutr. 2021. PMID: 33634219 Free PMC article.
-
Elucidating the sustained decline in under-three child linear growth faltering in Nepal, 1996-2016.Matern Child Nutr. 2022 Jan;18 Suppl 1(Suppl 1):e12982. doi: 10.1111/mcn.12982. Epub 2020 Mar 5. Matern Child Nutr. 2022. PMID: 32141213 Free PMC article.
-
Infant and young child feeding practices and child linear growth in Nepal: Regression-decomposition analysis of national survey data, 1996-2016.Matern Child Nutr. 2022 Jan;18 Suppl 1(Suppl 1):e12911. doi: 10.1111/mcn.12911. Epub 2020 Jan 10. Matern Child Nutr. 2022. PMID: 31922348 Free PMC article.
References
-
- Micronutrient Initiative. Investing in the future: a united call to action on vitamin and mineral deficiencies. Ottawa (Canada): Micronutrient Initiative;2009.
-
- Stevens GA, Bennett JE, Hennocq Q, Lu Y, De-Regil LM, Rogers L, Danaei G, Li G, White RA, Flaxman SR, et al. . Trends and mortality effects of vitamin A deficiency in children in 138 low-income and middle-income countries between 1991 and 2013: a pooled analysis of population-based surveys. Lancet Glob Health 2015;3(9):e528–36. - PubMed
-
- Stevens GA, Finucane MM, De-Regil LM, Paciorek CJ, Flaxman SR, Branca F, Peña-Rosas JP, Bhutta ZA, Ezzati M. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet Glob Health 2013;1(1):e16–25. - PMC - PubMed
-
- Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, de Onis M, Ezzati M, Grantham-McGregor S, Katz J, Martorell R. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013;382(9890):427–51. - PubMed
-
- WHO Global strategy for infant and young child feeding. Geneva (Switzerland): WHO;2003.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
