

Blood pressure variability predicts adverse events and cardiovascular outcomes in SPRINT
- PMID: 29984884
- PMCID: PMC8031192
- DOI: 10.1111/jch.13346
Blood pressure variability predicts adverse events and cardiovascular outcomes in SPRINT
Abstract
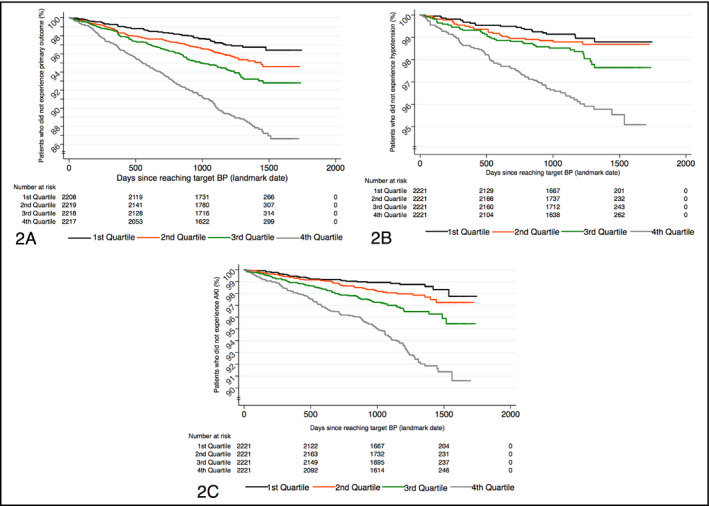
SPRINT (Systolic Blood Pressure Intervention Trial) highlighted the benefits of intensive targeted antihypertensive therapy but resulted in higher rates of treatment-related adverse events. Blood pressure (BP) variability has emerged as a significant predictor of outcomes over and above levels of BP. Using the SPRINT data set, we aimed to determine the relationship of BP variability with cardiovascular outcomes and side effects of antihypertensive therapy. The analyses included all participants randomized in SPRINT who reached the target systolic BP (SBP) for their respective groups (intensive < 120 mm Hg; standard < 140 mm Hg). Coefficients of variation (CV) for SBP, diastolic BP (DBP), and PP for each patient characterized variability. Student t test was used to compare treatment arms for each CV metric. Cox proportional hazards regression was used to identify independent predictors of the SPRINT primary outcome and adverse events. P < .15 on univariate analysis was required to enter the model and P < .05 to remain in it. A total of 8884 patients (4561 standard group; 4323 intensive group) met inclusion criteria. DBP CV differed between the groups (9.12 ± 3.20 standard group; 9.47 ± 3.49 intensive group [P < .0001]). DBP CV predicted a greater hazard for the primary outcome (hazard ratio [HR], 1.14) in the overall model as well as separate analyses by treatment arms (standard group HR, 1.15; intensive group HR, 1.19), each P < .0001. DBP CV also independently predicted a greater hazard for acute kidney injury (HR, 1.12) and hypotensive events (HR, 1.12). Visit-to-visit DBP variability independently predicted worse cardiovascular outcomes and hypoperfusion-related adverse events in SPRINT.
Keywords: blood pressure variability; cardiovascular outcomes; hypertension.
©2018 Wiley Periodicals, Inc.
Conflict of interest statement
All authors have no conflicts of interest to declare.
Figures

Comment in
-
Response to Letter to the Editor concerning manuscript, "Blood pressure variability predicts adverse events and cardiovascular outcomes in sprint".J Clin Hypertens (Greenwich). 2018 Nov;20(11):1646-1647. doi: 10.1111/jch.13400. Epub 2018 Oct 17. J Clin Hypertens (Greenwich). 2018. PMID: 30328256 Free PMC article. No abstract available.
-
Prognostic relevance of visit-to-visit office blood pressure variability in Systolic Blood Pressure Intervention Trial: Same data, different conclusions?J Clin Hypertens (Greenwich). 2018 Nov;20(11):1644-1645. doi: 10.1111/jch.13395. Epub 2018 Oct 17. J Clin Hypertens (Greenwich). 2018. PMID: 30328272 Free PMC article. No abstract available.
References
-
- Kearney PM, Whelton M, Reynolds K, et al. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217‐223. - PubMed
-
- Lewington S, Clarke R, Qizilbash N, et al. Age‐specific relevance of usual blood pressure to vascular mortality: a meta‐analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903‐1913. - PubMed
-
- MacMahon S, Peto R, Cutler J, et al. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet. 1990;335:765‐774. - PubMed
-
- O'Brien E, Asmar R, Beilin L, et al. Practice guidelines of the European Society of Hypertension for clinic, ambulatory and self BP measurement. J Hypertens 2005; 23: 697‐701. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
