

Rationale and design of the randomized multicentre His Optimized Pacing Evaluated for Heart Failure (HOPE-HF) trial
- PMID: 29984912
- PMCID: PMC6165934
- DOI: 10.1002/ehf2.12315
Rationale and design of the randomized multicentre His Optimized Pacing Evaluated for Heart Failure (HOPE-HF) trial
Abstract
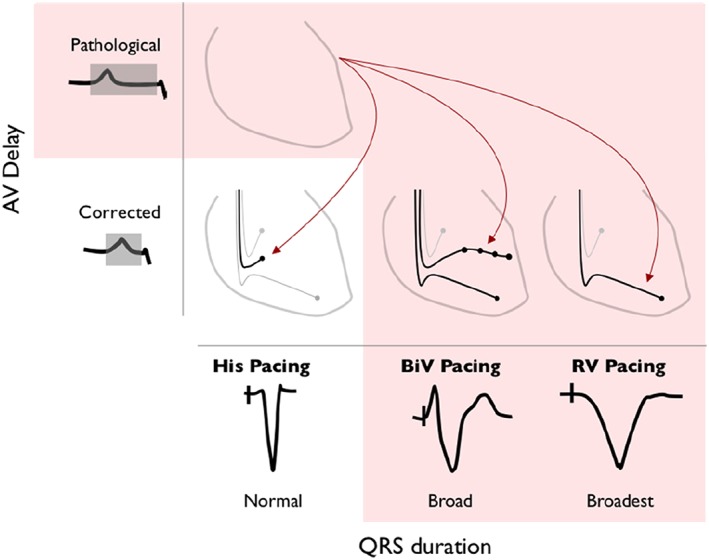
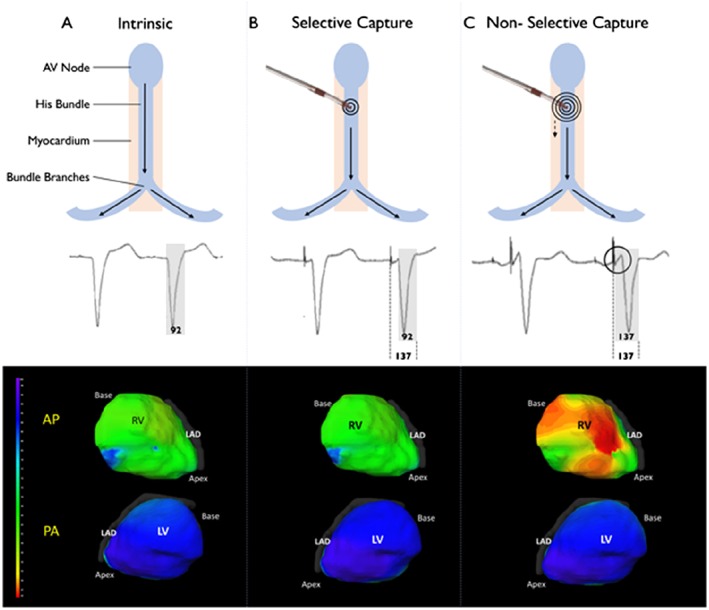
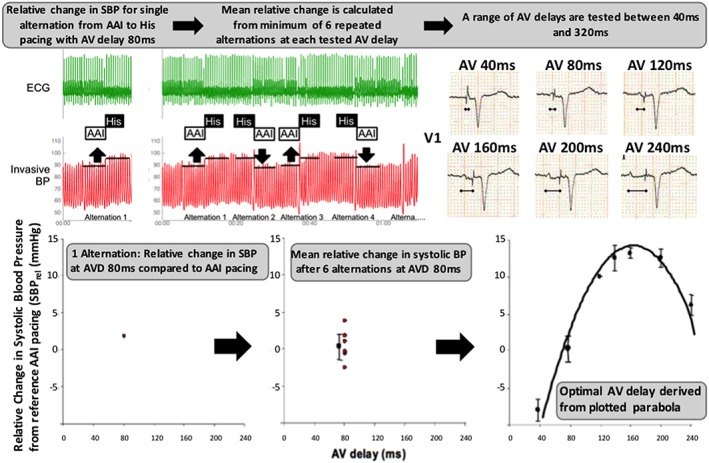
Aims: In patients with heart failure and a pathologically prolonged PR interval, left ventricular (LV) filling can be improved by shortening atrioventricular delay using His-bundle pacing. His-bundle pacing delivers physiological ventricular activation and has been shown to improve acute haemodynamic function in this group of patients. In the HOPE-HF (His Optimized Pacing Evaluated for Heart Failure) trial, we are investigating whether these acute haemodynamic improvements translate into improvements in exercise capacity and heart failure symptoms.
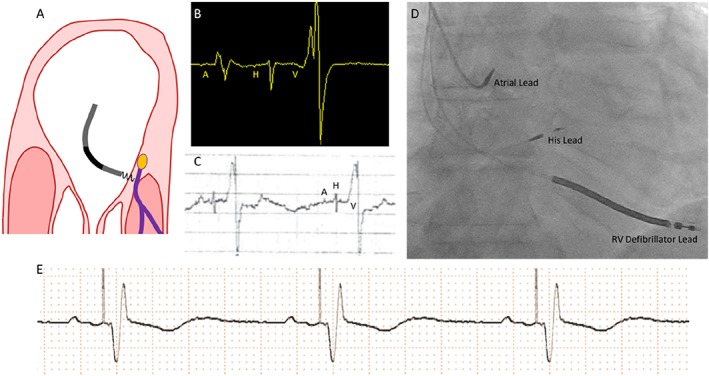
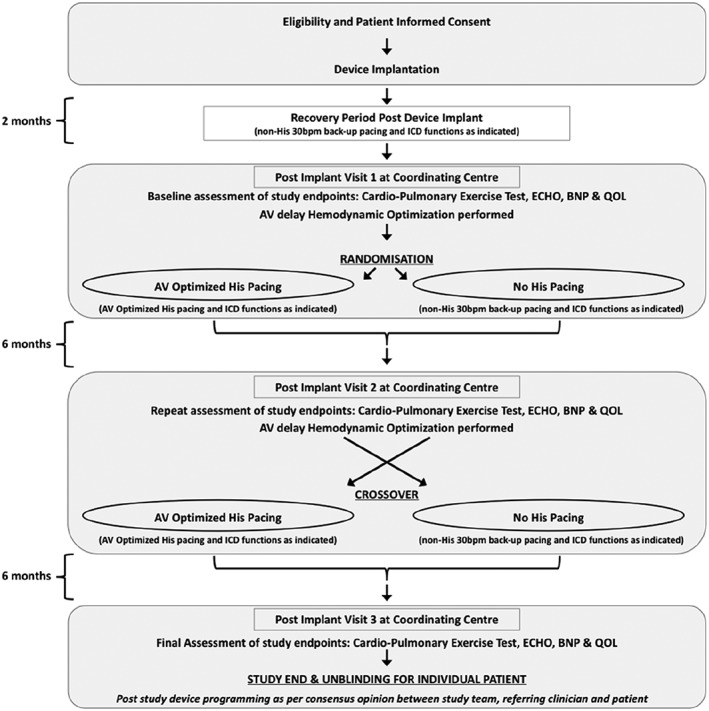
Methods and results: This multicentre, double-blind, randomized, crossover study aims to randomize 160 patients with PR prolongation (≥200 ms), LV impairment (EF ≤ 40%), and either narrow QRS (≤140 ms) or right bundle branch block. All patients receive a cardiac device with leads positioned in the right atrium and the His bundle. Eligible patients also receive a defibrillator lead. Those not eligible for implantable cardioverter defibrillator have a backup pacing lead positioned in an LV branch of the coronary sinus. Patients are allocated in random order to 6 months of (i) haemodynamically optimized dual chamber His-bundle pacing and (ii) backup pacing only, using the non-His ventricular lead. The primary endpoint is change in exercise capacity assessed by peak oxygen uptake. Secondary endpoints include change in ejection fraction, quality of life scores, B-type natriuretic peptide, daily patient activity levels, and safety and feasibility assessments of His-bundle pacing.
Conclusions: Hope-HF aims to determine whether correcting PR prolongation in patients with heart failure and narrow QRS or right bundle branch block using haemodynamically optimized dual chamber His-bundle pacing improves exercise capacity and symptoms. We aim to complete recruitment by the end of 2018 and report in 2020.
Keywords: Atrioventricular delay; Heart failure; His-bundle pacing; Optimization.
© 2018 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Figures
References
-
- Stockburger M, Moss AJ, Klein HU, Zareba W, Goldenberg I, Biton Y, McNitt S, Kutyifa V. Sustained clinical benefit of cardiac resynchronization therapy in non‐LBBB patients with prolonged PR‐interval: MADIT‐CRT long‐term follow‐up. Clin Res Cardiol 2016; 105: 944–952. - PubMed
-
- Kutyifa V, Stockburger M, Daubert JP, Holmqvist F, Olshansky B, Schuger C, Klein H, Goldenberg I, Brenyo A, McNitt S, Merkely B, Zareba W, Moss AJ. PR interval identifies clinical response in patients with non‐left bundle branch block: a Multicenter Automatic Defibrillator Implantation Trial‐Cardiac Resynchronization Therapy substudy. Circ Arrhythm Electrophysiol 2014; 7: 645–651. - PubMed
-
- Ploux S, Eschalier R, Whinnett ZI, Lumens J, Derval N, Sacher F, Hocini M, Jaïs P, Dubois R, Ritter P, Haïssaguerre M, Wilkoff BL, Francis DP, Bordachar P. Electrical dyssynchrony induced by biventricular pacing: implications for patient selection and therapy improvement. Heart Rhythm 2015; 12: 782–791. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
