

The cardiac lymphatic system stimulates resolution of inflammation following myocardial infarction
- PMID: 29985167
- PMCID: PMC6063482
- DOI: 10.1172/JCI97192
The cardiac lymphatic system stimulates resolution of inflammation following myocardial infarction
Abstract
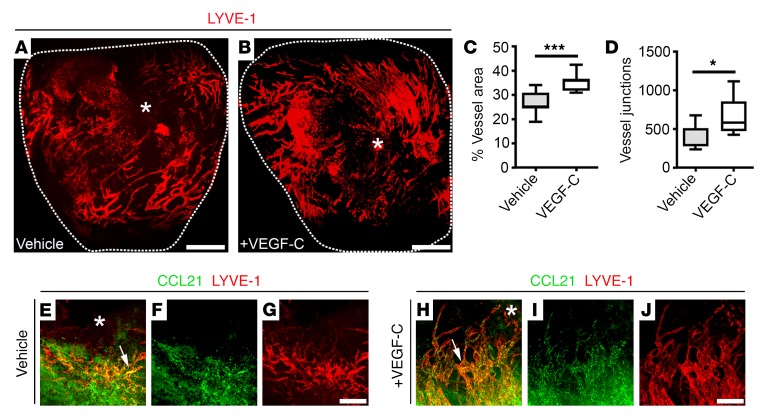
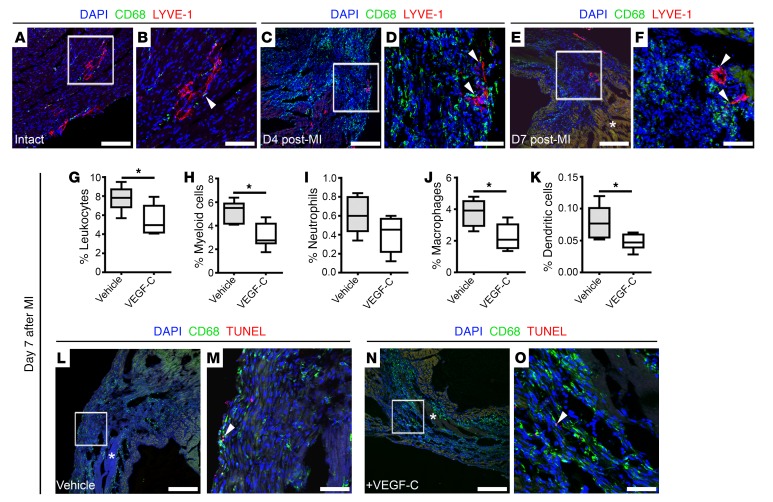
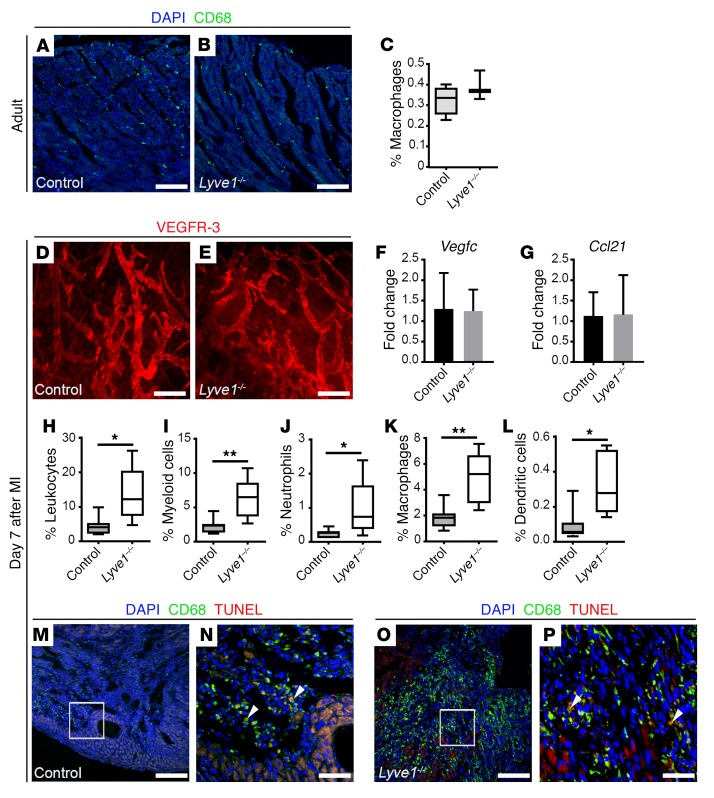
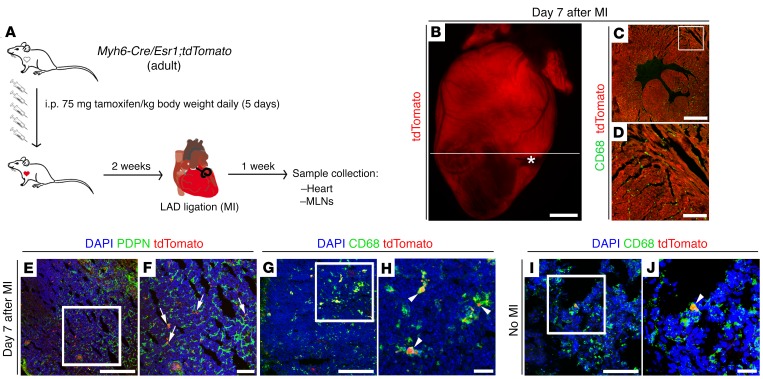
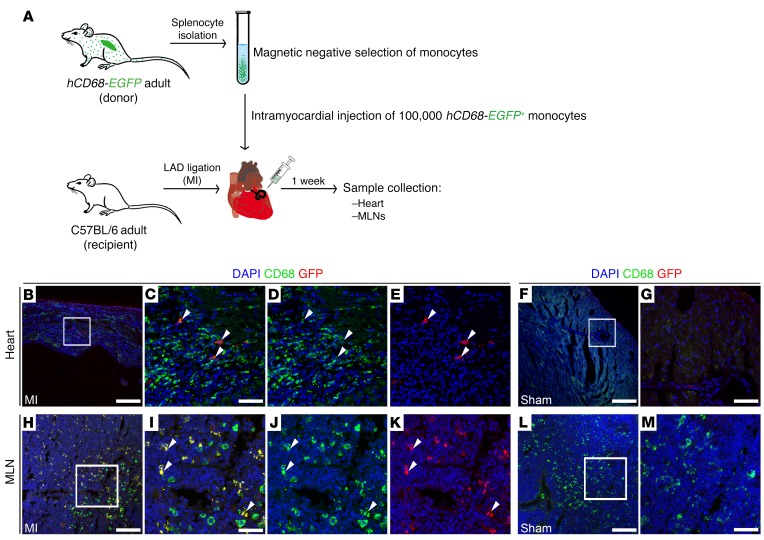
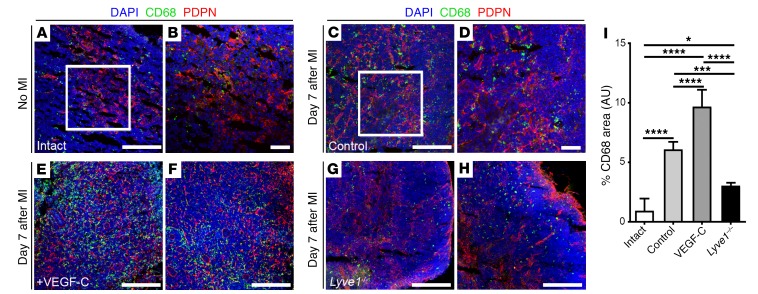
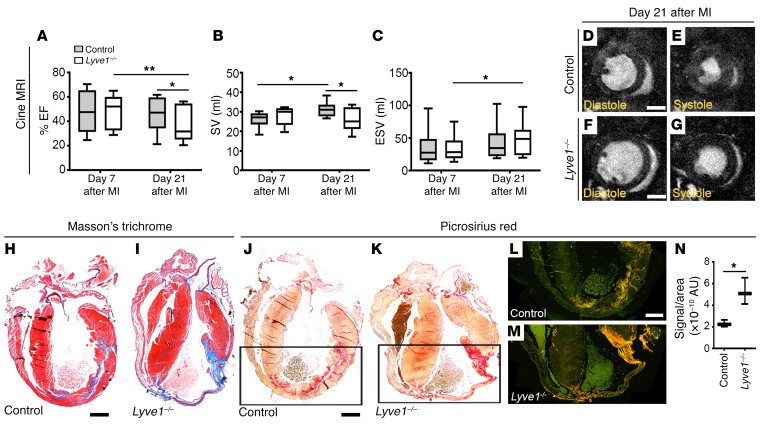
Myocardial infarction (MI) arising from obstruction of the coronary circulation engenders massive cardiomyocyte loss and replacement by non-contractile scar tissue, leading to pathological remodeling, dysfunction, and ultimately heart failure. This is presently a global health problem for which there is no effective cure. Following MI, the innate immune system directs the phagocytosis of dead cell debris in an effort to stimulate cell repopulation and tissue renewal. In the mammalian adult heart, however, the persistent influx of immune cells, coupled with the lack of an inherent regenerative capacity, results in cardiac fibrosis. Here, we reveal that stimulation of cardiac lymphangiogenesis with VEGF-C improves clearance of the acute inflammatory response after MI by trafficking immune cells to draining mediastinal lymph nodes (MLNs) in a process dependent on lymphatic vessel endothelial hyaluronan receptor 1 (LYVE-1). Deletion of Lyve1 in mice, preventing docking and transit of leukocytes through the lymphatic endothelium, results in exacerbation of chronic inflammation and long-term deterioration of cardiac function. Our findings support targeting of the lymphatic/immune cell axis as a therapeutic paradigm to promote immune modulation and heart repair.
Keywords: Cardiovascular disease; Inflammation; Vascular Biology.
Conflict of interest statement
Figures
Comment in
-
Cardiac lymphatics mediate the resolution of inflammation.Nat Rev Cardiol. 2018 Oct;15(10):583. doi: 10.1038/s41569-018-0067-z. Nat Rev Cardiol. 2018. PMID: 30042432 No abstract available.
-
The lymphatic border patrol outwits inflammatory cells in myocardial infarction.Sci Transl Med. 2018 Jul 25;10(451):eaau7379. doi: 10.1126/scitranslmed.aau7379. Sci Transl Med. 2018. PMID: 30774753 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
