

Development and clinical validity of a novel blood-based molecular biomarker for subclinical acute rejection following kidney transplant
- PMID: 29985559
- PMCID: PMC6387870
- DOI: 10.1111/ajt.15011
Development and clinical validity of a novel blood-based molecular biomarker for subclinical acute rejection following kidney transplant
Abstract
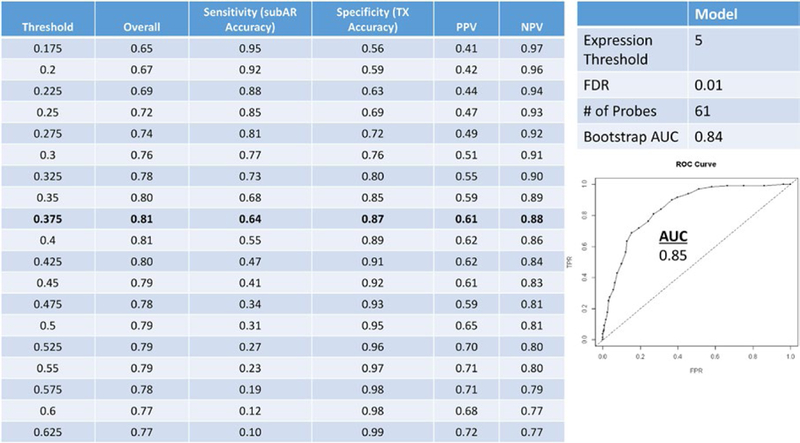
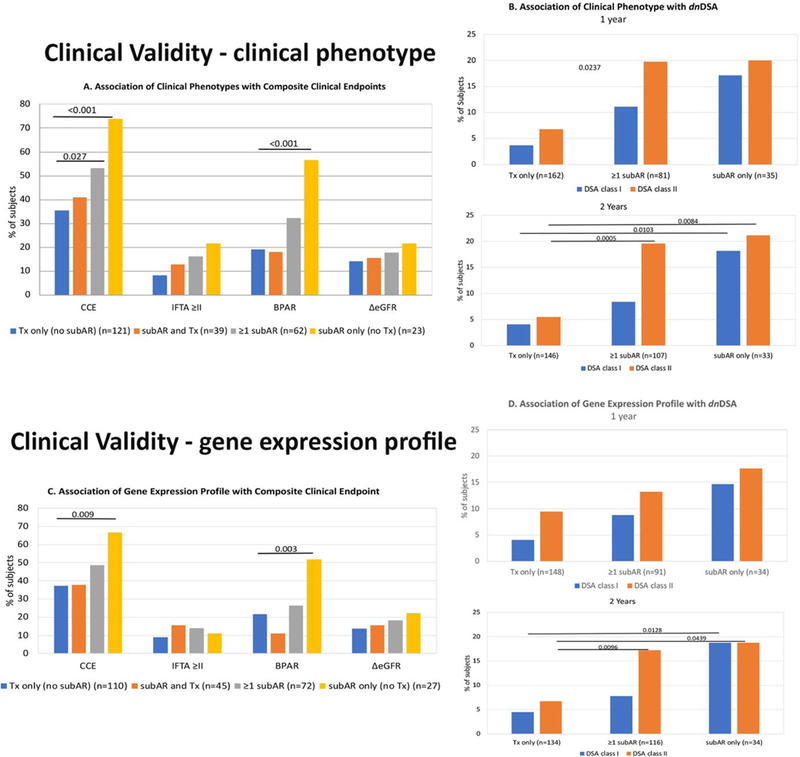
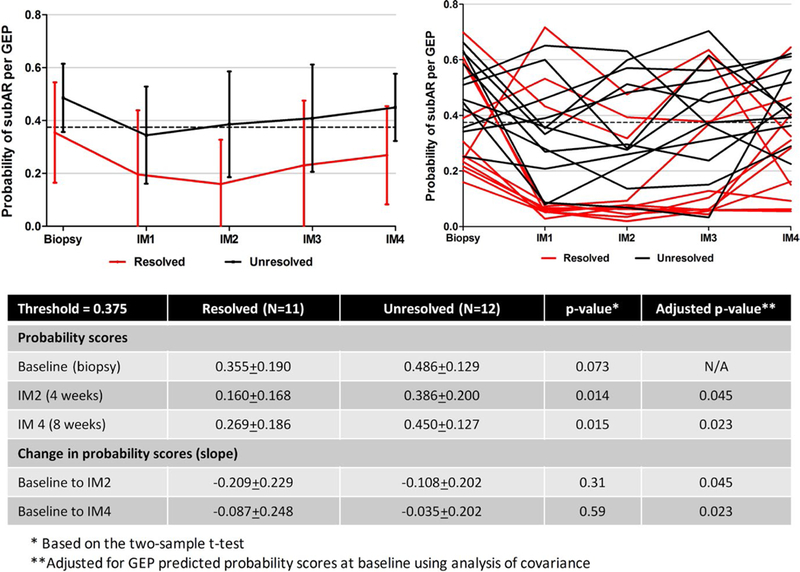
Noninvasive biomarkers are needed to monitor stable patients after kidney transplant (KT), because subclinical acute rejection (subAR), currently detectable only with surveillance biopsies, can lead to chronic rejection and graft loss. We conducted a multicenter study to develop a blood-based molecular biomarker for subAR using peripheral blood paired with surveillance biopsies and strict clinical phenotyping algorithms for discovery and validation. At a predefined threshold, 72% to 75% of KT recipients achieved a negative biomarker test correlating with the absence of subAR (negative predictive value: 78%-88%), while a positive test was obtained in 25% to 28% correlating with the presence of subAR (positive predictive value: 47%-61%). The clinical phenotype and biomarker independently and statistically correlated with a composite clinical endpoint (renal function, biopsy-proved acute rejection, ≥grade 2 interstitial fibrosis, and tubular atrophy), as well as with de novo donor-specific antibodies. We also found that <50% showed histologic improvement of subAR on follow-up biopsies despite treatment and that the biomarker could predict this outcome. Our data suggest that a blood-based biomarker that reduces the need for the indiscriminate use of invasive surveillance biopsies and that correlates with transplant outcomes could be used to monitor KT recipients with stable renal function, including after treatment for subAR, potentially improving KT outcomes.
Keywords: alloantibody; biomarker; clinical research/practice; clinical trial; genomics; kidney transplantation/nephrology; rejection: subclinical; translational research/science.
© 2018 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
DISCLOSURE
The authors of this manuscript have conflicts of interest to disclose as described by the
Figures
Comment in
-
The special relativity of noninvasive biomarkers for acute rejection.Am J Transplant. 2019 Jan;19(1):5-8. doi: 10.1111/ajt.15078. Epub 2018 Sep 17. Am J Transplant. 2019. PMID: 30125470 No abstract available.
-
Clinical implications for the use of a biomarker for subclinical rejection - Conflating arguments cause a disconnection between the premise and the conclusion.Am J Transplant. 2019 Jul;19(7):2141-2142. doi: 10.1111/ajt.15327. Epub 2019 Mar 18. Am J Transplant. 2019. PMID: 30809931 No abstract available.
References
-
- Tonelli M, Wiebe N, Knoll G, et al. Systematic review: kidney trans¬plantation compared with dialysis in clinically relevant outcomes. Am J Transplant. 2011;11(10):2093–2109. - PubMed
-
- US Renal Data System. 2016 USRDS annual data report: Epidemiology of kidney disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2016.
-
- Meier-Kriesche HU, Schold JD, Srinivas TR, Kaplan B. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant. 2004;4(3):378–383. - PubMed
-
- Nankivell BJ, Chapman JR. The significance of subclinical rejection and the value of protocol biopsies. Am J Transplant. 2006;6(9):2006–2012. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
