

Assessment of facility readiness for implementing the WHO/UNICEF standards for improving quality of maternal and newborn care in health facilities - experiences from UNICEF's implementation in three countries of South Asia and sub-Saharan Africa
- PMID: 29986692
- PMCID: PMC6038273
- DOI: 10.1186/s12913-018-3334-0
Assessment of facility readiness for implementing the WHO/UNICEF standards for improving quality of maternal and newborn care in health facilities - experiences from UNICEF's implementation in three countries of South Asia and sub-Saharan Africa
Abstract
Background: There is a global drive to promote facility deliveries but unless coupled with concurrent improvement in care quality, it might not translate into mortality reduction for mothers and babies. The World Health Organization published the new "Standards for improving quality of care for mothers and newborns in health facilities" but these have not been tested in low- and middle-income settings. UNICEF and its partners are taking the advantage provided by the Mother and Baby Friendly Hospital Initiative in Bangladesh, Ghana and Tanzania to test these standards to inform country adaptation. This manuscript presents a framework used for assessment of facility quality of care to inform the effect of quality improvement interventions.
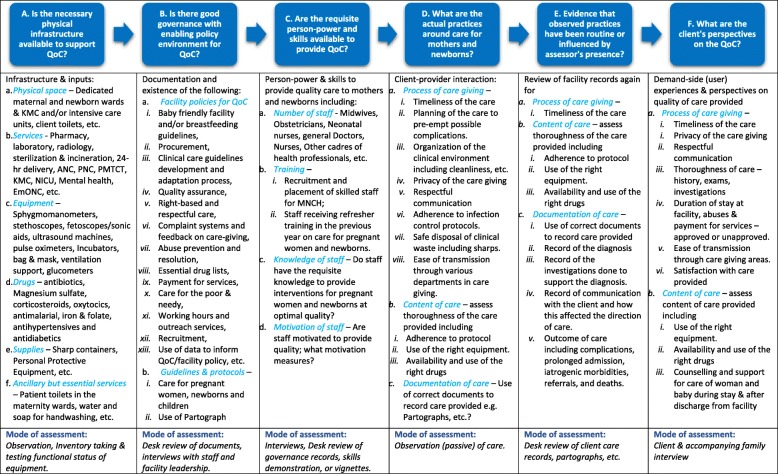
Methods: This assessment employed a quasi-experimental design with pre-post assessments in "implementation" and "comparison" facilities-the latter will have no quality improvement interventions implemented. UNICEF and assessment partners developed an assessment framework, developed uniform data collection tools and manuals for harmonised training and implementation across countries. The framework involves six modules assessing: facility structures, equipment, drugs and supplies; policies and guidelines supporting care-giving, staff recruitment and training; care-providers competencies; previous medical records; provider-client interactions (direct observation); and client perspectives on care quality; using semi-structured questionnaires and data collectors with requisite training. In Bangladesh, the assessment was conducted in 3 districts. In one "intervention" district, the district hospital and five upazilla health complexes were assessed. similar number of facilities were assessed each two adjoining comparison districts. In Ghana it was in three hospitals and five health centres and in Tanzania, two hospitals and four health centres. In the latter countries, same number of facilities were selected in the same number of districts to serve for comparison. Outcomes were structured to examine whether facilities currently provide services commensurate with their designation (basic or comprehensive emergency obstetric and newborn care). These outcomes were stratified so that they inform intervention implementation in the short-, medium- and long-term.
Conclusion: This strategy and framework provides a very useful model for supporting country implementation of the new WHO standards. It will serve as a template around which countries can build quality of care assessment strategies and metrics to inform their health systems on the effect of QI interventions on care processes and outcomes.
Conflict of interest statement
Ethics approval and consent to participate
Prior to the onset of the assessment, country-specific adaptations of the study protocol have been approved by the Ethics Committee and Institutional Review Boards of the International Centre for Diarrhoeal Diseases Research (Bangladesh); Navrongo Health Research Centre of the Ghana Health Service (Ghana) and the National Institute of Medical Research (Tanzania). The approval also included references to allow for pooling of data across all three countries for analysis.
This is an observational study in which pregnant women presenting in labour within the health facilities, health facility staff and managers are being observed or interviewed. There are no conceivable direct safety concerns. Mothers having a still birth or newborn death will be excluded from interviews to avoid distress to already traumatized individuals. Observation of care might involve invading the privacy of the patient and might be distressing to the care provider but participants will be reassured before the observations begin. Each respondent was individually consented for participation in the study. Facility staff were also assured that the study is not a fault-finding mission and assured that any information they provide or that will be collected on their practices will be confidential and will not affect their position within the facility or in the health services. Data collectors read out a standard study information sheet and the consent form to all respondents in a language of their preference and checked for understanding before a request was made for consent. Participation will be voluntary with assurance of participants’ rights to withdraw from the assessment at any stage, even after initial consent. Agreement to participate in the study was indicated by a signature or a thumbprint. Confidentiality of all data collected is being maintained, always, and accessible only to senior project staff and to the study coordinators. The database is being stored on a security protected server, with password access only by senior project staff. The data forms are being stored in secure storage to be kept for a set minimum period agreed between UNICEF and the respective countries after the end of the study. Analyses will present aggregate results without identifier information. All interviews are being conducted in the respondents’ preferred language. For the qualitative interviews, consent is being taken for recording the interview.
Consent for publication
Not applicable.
Competing interests
One co-author, Debra Jackson, was an editor of this journal till April 2018 but the decision and process of submission was completely transparent and all the authors declare no conflict of or competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Health Organization . Trends in maternal mortality: 1990-2013. Geneva: World Health Organization; 2014.
-
- UN Inter-agency Group for Child Mortality Estimation (IGME) Levels and trends in child mortality: Report 2013. New York: UNICEF; 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
