

Cross-sex Hormones and Acute Cardiovascular Events in Transgender Persons: A Cohort Study
- PMID: 29987313
- PMCID: PMC6636681
- DOI: 10.7326/M17-2785
Cross-sex Hormones and Acute Cardiovascular Events in Transgender Persons: A Cohort Study
Abstract
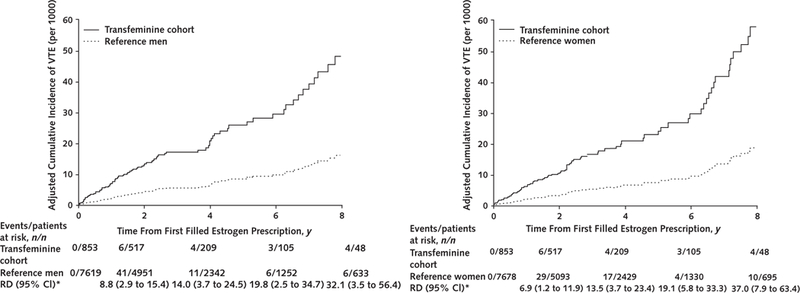
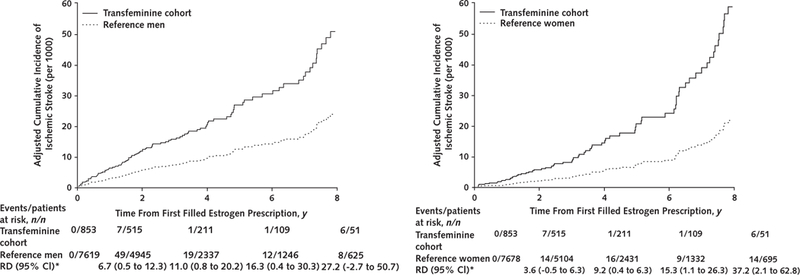
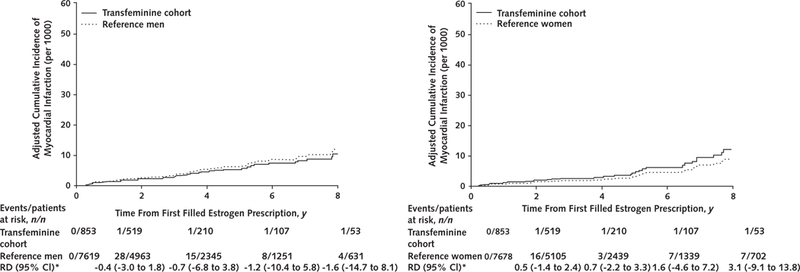
Background: Venous thromboembolism (VTE), ischemic stroke, and myocardial infarction in transgender persons may be related to hormone use.
Objective: To examine the incidence of these events in a cohort of transgender persons.
Design: Electronic medical record-based cohort study of transgender members of integrated health care systems who had an index date (first evidence of transgender status) from 2006 through 2014. Ten male and 10 female cisgender enrollees were matched to each transgender participant by year of birth, race/ethnicity, study site, and index date enrollment.
Setting: Kaiser Permanente in Georgia and northern and southern California.
Patients: 2842 transfeminine and 2118 transmasculine members with a mean follow-up of 4.0 and 3.6 years, respectively, matched to 48 686 cisgender men and 48 775 cisgender women.
Measurements: VTE, ischemic stroke, and myocardial infarction events ascertained from diagnostic codes through the end of 2016 in transgender and reference cohorts.
Results: Transfeminine participants had a higher incidence of VTE, with 2- and 8-year risk differences of 4.1 (95% CI, 1.6 to 6.7) and 16.7 (CI, 6.4 to 27.5) per 1000 persons relative to cisgender men and 3.4 (CI, 1.1 to 5.6) and 13.7 (CI, 4.1 to 22.7) relative to cisgender women. The overall analyses for ischemic stroke and myocardial infarction demonstrated similar incidence across groups. More pronounced differences for VTE and ischemic stroke were observed among transfeminine participants who initiated hormone therapy during follow-up. The evidence was insufficient to allow conclusions regarding risk among transmasculine participants.
Limitation: Inability to determine which transgender members received hormones elsewhere.
Conclusion: The patterns of increases in VTE and ischemic stroke rates among transfeminine persons are not consistent with those observed in cisgender women. These results may indicate the need for long-term vigilance in identifying vascular side effects of cross-sex estrogen.
Primary funding source: Patient-Centered Outcomes Research Institute and Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Figures
Comment in
-
Study Finds Increased Venous Thromboembolism Risk in Transfeminine Patients.Am J Nurs. 2018 Oct;118(10):69. doi: 10.1097/01.NAJ.0000546383.12045.1d. Am J Nurs. 2018. PMID: 30260889 No abstract available.
-
Cross-Sex Hormones and Acute Cardiovascular Events in Transgender Persons.Ann Intern Med. 2019 Jan 15;170(2):142-143. doi: 10.7326/L18-0563. Ann Intern Med. 2019. PMID: 30641564 No abstract available.
-
Cross-Sex Hormones and Acute Cardiovascular Events in Transgender Persons.Ann Intern Med. 2019 Jan 15;170(2):143. doi: 10.7326/L18-0564. Ann Intern Med. 2019. PMID: 30641565 No abstract available.
References
-
- Bockting W From construction to context: gender through the eyes of the transgendered. SIECUS Rep. 1999;28:3–7.
-
- Knudson G, De Cuypere G, Bockting W. Recommendations for revision of the DSM diagnoses of gender identity disorders: consensus statement of the World Professional Association for Transgender Health. Int J Transgend. 2010;12:115–8.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical