

Somatic mutations precede acute myeloid leukemia years before diagnosis
- PMID: 29988143
- PMCID: PMC6849383
- DOI: 10.1038/s41591-018-0081-z
Somatic mutations precede acute myeloid leukemia years before diagnosis
Abstract
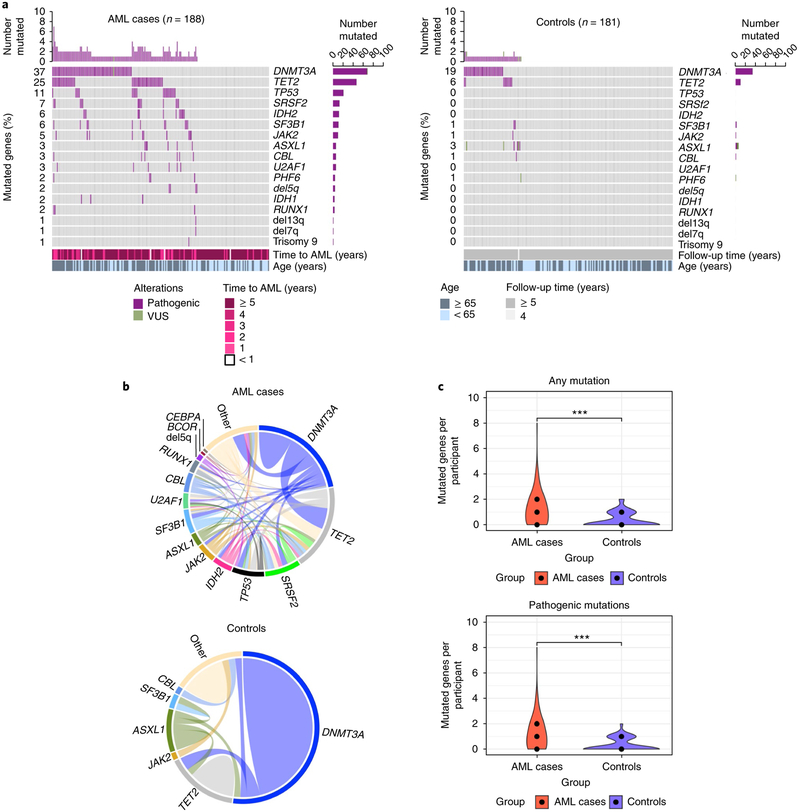
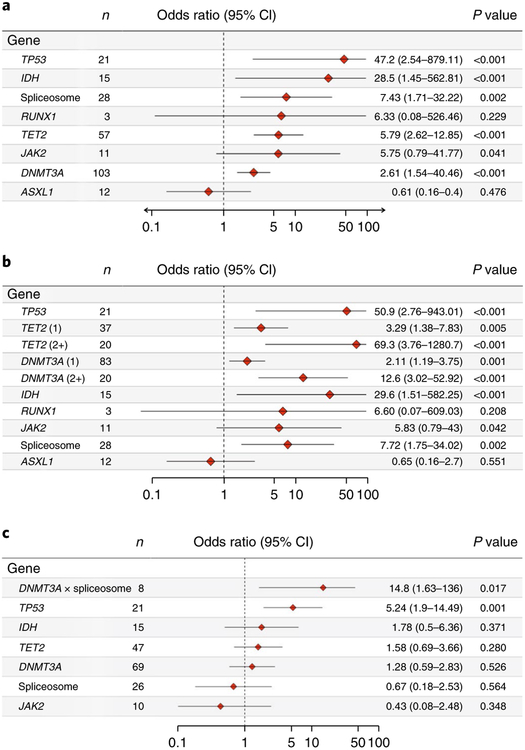
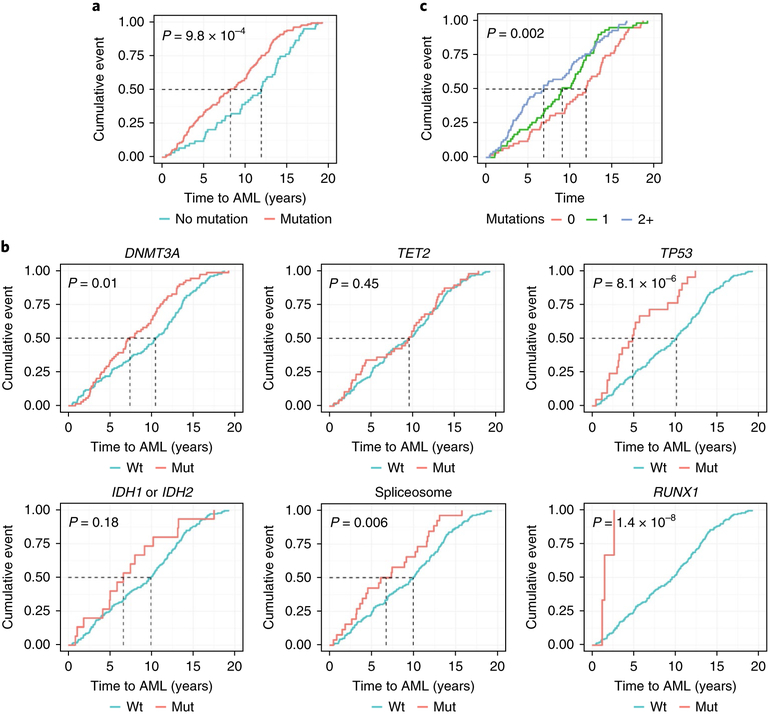
The pattern of somatic mutations observed at diagnosis of acute myeloid leukemia (AML) has been well-characterized. However, the premalignant mutational landscape of AML and its impact on risk and time to diagnosis is unknown. Here we identified 212 women from the Women's Health Initiative who were healthy at study baseline, but eventually developed AML during follow-up (median time: 9.6 years). Deep sequencing was performed on peripheral blood DNA of these cases and compared to age-matched controls that did not develop AML. We discovered that mutations in IDH1, IDH2, TP53, DNMT3A, TET2 and spliceosome genes significantly increased the odds of developing AML. All subjects with TP53 mutations (n = 21 out of 21 patients) and IDH1 and IDH2 (n = 15 out of 15 patients) mutations eventually developed AML in our study. The presence of detectable mutations years before diagnosis suggests that there is a period of latency that precedes AML during which early detection, monitoring and interventional studies should be considered.
Conflict of interest statement
Competing interests
The authors declares no competing interests.
Figures


Comment in
-
Predicting progression to AML.Nat Med. 2018 Jul;24(7):904-906. doi: 10.1038/s41591-018-0114-7. Nat Med. 2018. PMID: 29988142 No abstract available.
-
Roots of AML Detectable Long before Symptoms.Cancer Discov. 2018 Sep;8(9):1056. doi: 10.1158/2159-8290.CD-NB2018-099. Epub 2018 Jul 23. Cancer Discov. 2018. PMID: 30037845
-
Early prediction of AML risk.Nat Rev Clin Oncol. 2018 Oct;15(10):590. doi: 10.1038/s41571-018-0078-z. Nat Rev Clin Oncol. 2018. PMID: 30050093 No abstract available.
-
How to predict the future.Nat Rev Cancer. 2018 Sep;18(9):529. doi: 10.1038/s41568-018-0046-z. Nat Rev Cancer. 2018. PMID: 30050149 No abstract available.
-
How to predict the future.Nat Rev Genet. 2018 Sep;19(9):531. doi: 10.1038/s41576-018-0041-y. Nat Rev Genet. 2018. PMID: 30054567 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
