

Orally-transmitted Chagas disease: Epidemiological, clinical, serological and molecular outcomes of a school microepidemic in Chichiriviche de la Costa, Venezuela
- PMID: 29988179
- PMCID: PMC5991850
- DOI: 10.1016/j.parepi.2016.02.005
Orally-transmitted Chagas disease: Epidemiological, clinical, serological and molecular outcomes of a school microepidemic in Chichiriviche de la Costa, Venezuela
Abstract
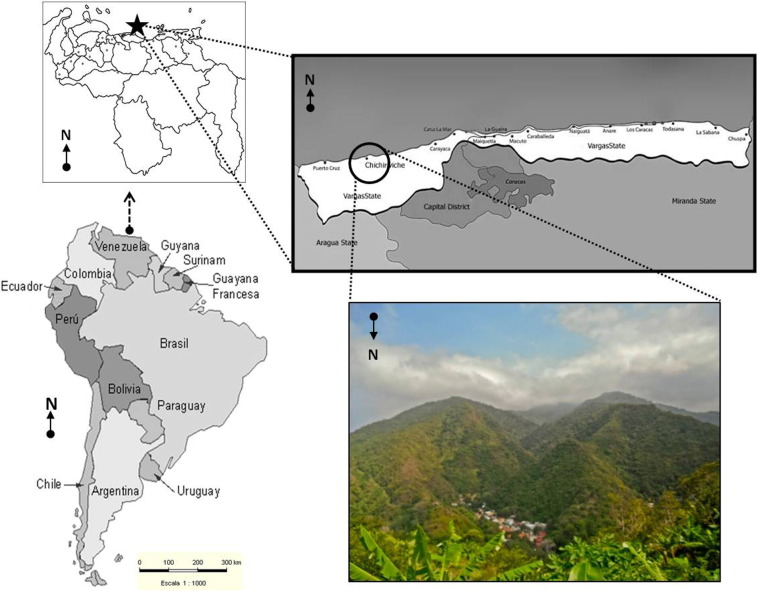
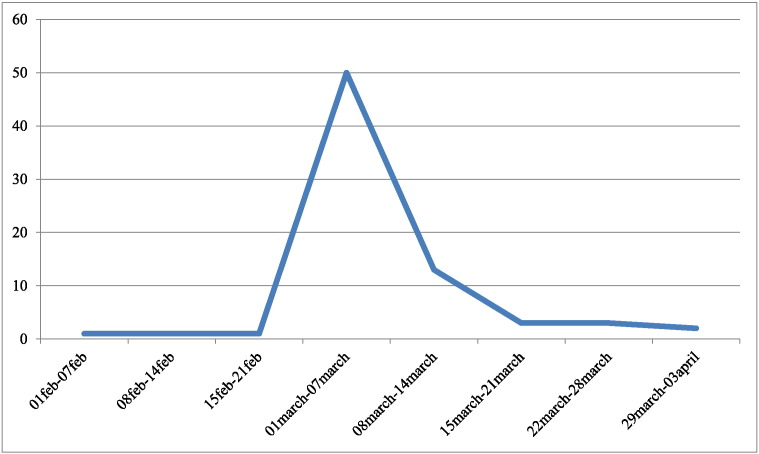
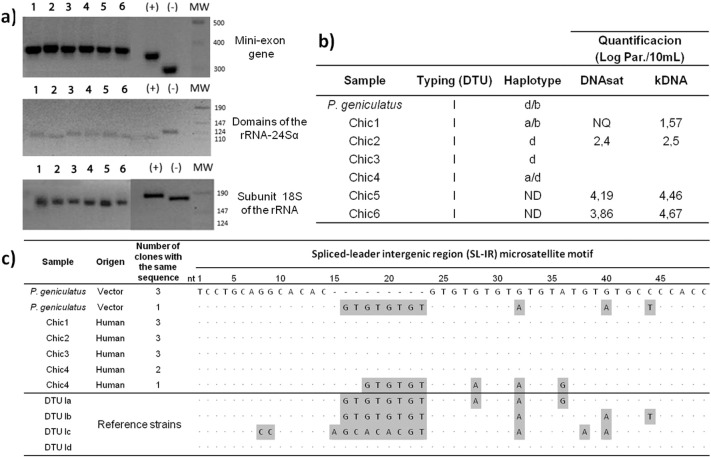
Oral transmission of Trypanosoma cruzi is a frequent cause of acute Chagas disease (ChD). In the present cross-sectional study, we report the epidemiological, clinical, serological and molecular outcomes of the second largest outbreak of oral ChD described in the literature. It occurred in March 2009 in Chichiriviche de la Costa, a rural seashore community at the central littoral in Venezuela. The vehicle was an artisanal guava juice prepared at the local school and Panstrongylus geniculatus was the vector involved. TcI genotype was isolated from patients and vector; some showed a mixture of haplotypes. Using molecular markers, parasitic loads were high. Eighty-nine cases were diagnosed, the majority (87.5%) in school children 6-15 years of age. Frequency of symptomatic patients was high (89.9%) with long-standing fever in 87.5%; 82.3% had pericardial effusion detected by echocardiogram and 41% had EKG abnormalities. Three children, a pregnant woman and her stillborn child died (5.6% mortality). The community was addressed by simultaneous determination of specific IgG and IgM, confirmed with indirect hemagglutination and lytic antibodies. Determination of IgG and IgA in saliva had low sensitivity. No individual parasitological or serological technique diagnosed 100% of cases. Culture and PCR detected T. cruzi in 95.5% of examined individuals. Based on the increasing incidence of oral acute cases of ChD, it appears that food is becoming one of the most important modes of transmission in the Amazon, Caribbean and Andes regions of America.
Keywords: Chagas disease; Chichiriviche de la Costa; Foodborne; Oral transmission; Saliva; Venezuela.
Figures


References
-
- Pinto A.Y.N., Valente S.A.S., Valente V.C., Ferreira Junior A.G., Coura J.R. Fase aguda da doença de Chagas na Amazônia brasileira. Estudo de 233 casos no Pará, Amapá e Maranhão observados entre 1988 e 2005. Rev. Soc. Bras. Med. Trop. 2008;41:602–614. - PubMed
-
- Shikanai-Yasuda M.A., Carvalho N.B. Oral transmission of Chagas disease. Clin. Infect. Dis. 2012;54:845–852. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
