

Streptococcus pneumoniae's Virulence and Host Immunity: Aging, Diagnostics, and Prevention
- PMID: 29988379
- PMCID: PMC6023974
- DOI: 10.3389/fimmu.2018.01366
Streptococcus pneumoniae's Virulence and Host Immunity: Aging, Diagnostics, and Prevention
Abstract
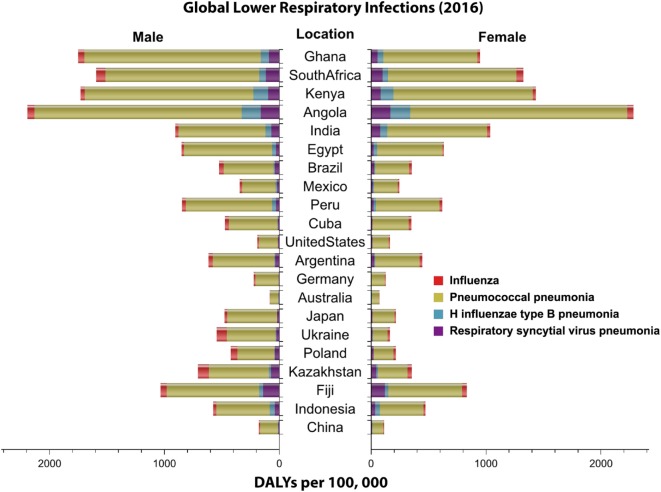
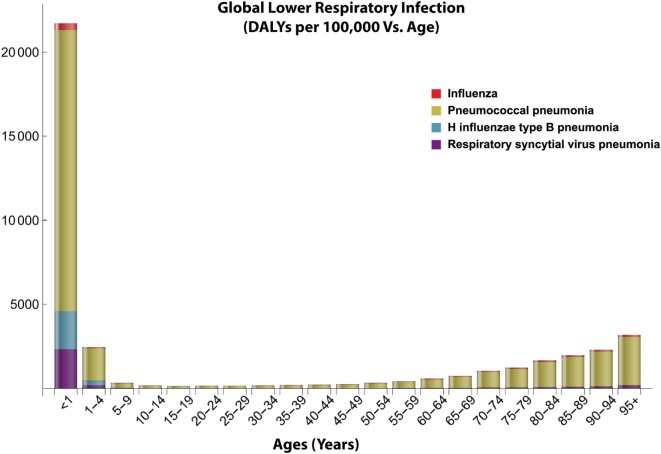
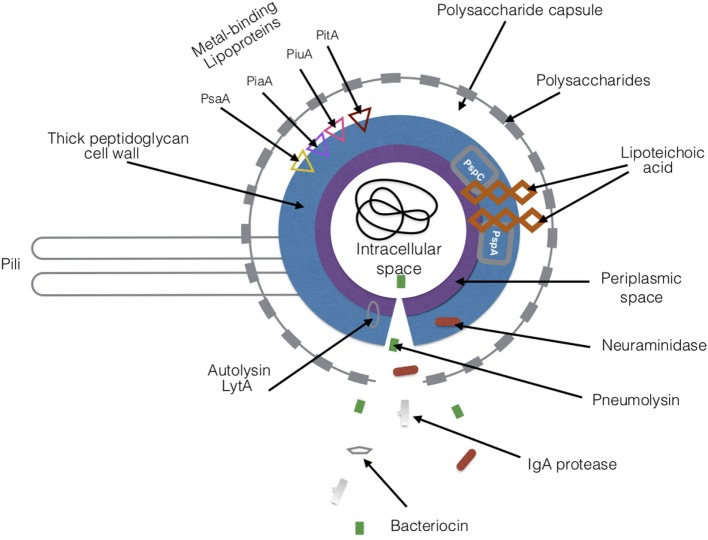
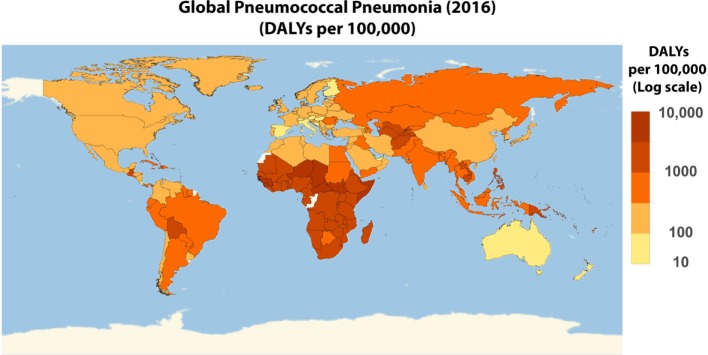
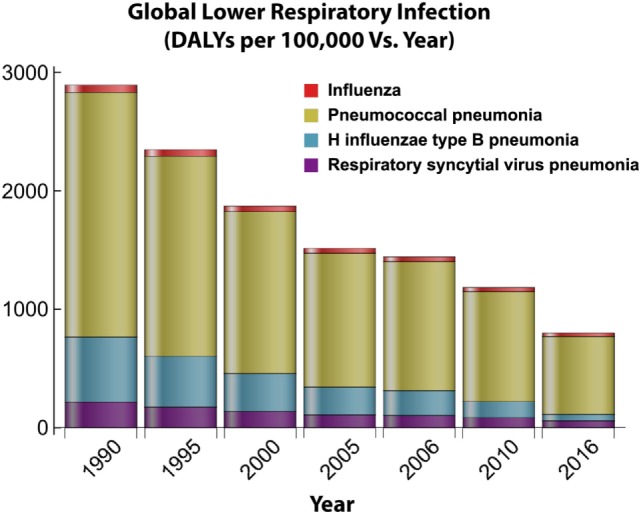
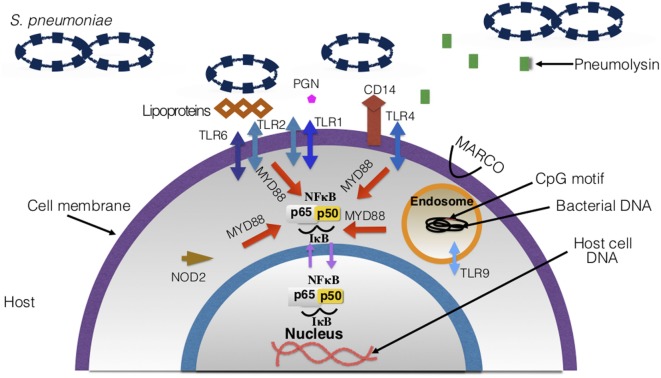
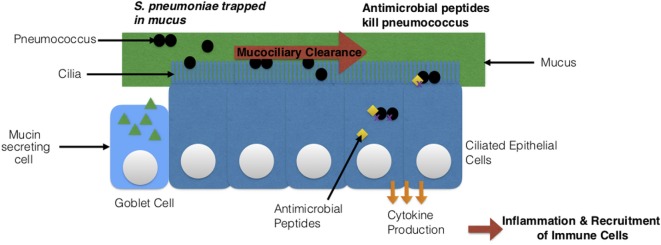
Streptococcus pneumoniae is an infectious pathogen responsible for millions of deaths worldwide. Diseases caused by this bacterium are classified as pneumococcal diseases. This pathogen colonizes the nasopharynx of its host asymptomatically, but overtime can migrate to sterile tissues and organs and cause infections. Pneumonia is currently the most common pneumococcal disease. Pneumococcal pneumonia is a global health concern and vastly affects children under the age of five as well as the elderly and individuals with pre-existing health conditions. S. pneumoniae has a large selection of virulence factors that promote adherence, invasion of host tissues, and allows it to escape host immune defenses. A clear understanding of S. pneumoniae's virulence factors, host immune responses, and examining the current techniques available for diagnosis, treatment, and disease prevention will allow for better regulation of the pathogen and its diseases. In terms of disease prevention, other considerations must include the effects of age on responses to vaccines and vaccine efficacy. Ongoing work aims to improve on current vaccination paradigms by including the use of serotype-independent vaccines, such as protein and whole cell vaccines. Extending our knowledge of the biology of, and associated host immune response to S. pneumoniae is paramount for our improvement of pneumococcal disease diagnosis, treatment, and improvement of patient outlook.
Keywords: immunology; pathogenesis; pneumococcal; respiratory; virulence.
Figures
References
-
- Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis (2007) 44(Suppl 2):S27–72.10.1086/511159 - DOI - PMC - PubMed
-
- Mayo Clinic Staff. Infectious Diseases. Mayo Foundation for Medical Education and Research; (2016). Available from: https://www.mayoclinic.org/diseases-conditions/infectious-diseases/sympt... (Accessed: March 26, 2017).
-
- Dasaraju PV, Liu C. Chapter 93 – Infections of the respiratory system. In: Baron S, editor. Med Microbiol 4th ed Galveston, TX: University of Texas Medical Branch; (1996). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources