

Disparities in caesarean section prevalence and determinants across sub-Saharan Africa countries
- PMID: 29988650
- PMCID: PMC6027740
- DOI: 10.1186/s41256-018-0074-y
Disparities in caesarean section prevalence and determinants across sub-Saharan Africa countries
Abstract
Background: Access to safe Cesarean section (C-section) in resource-constrained settings such as sub-Sahara Africa (SSA) region is a foremost approach to reduce maternal mortality. C-section is an obstetric operative procedure used appropriately to improve delivery outcomes. However, errors in the procedure have enormous potential harm that may outweigh the benefits. This study assessed the prevalence and determinants of C-section in several SSA countries. This study examined the prevalence and determinants associated with cesarean delivery in SSA countries.
Methods: Secondary data of women of reproductive age (15-49 years) from the current Demographic and Health Survey (DHS) in 34 SSA countries was utilized in this study. The mode of delivery among women was the primary outcome variable. Percentage and descriptive statistics were used to conduct univariate analyses. Furthermore, multivariable multilevel logistic regression was used to investigate correlates of C-section among SSA women.
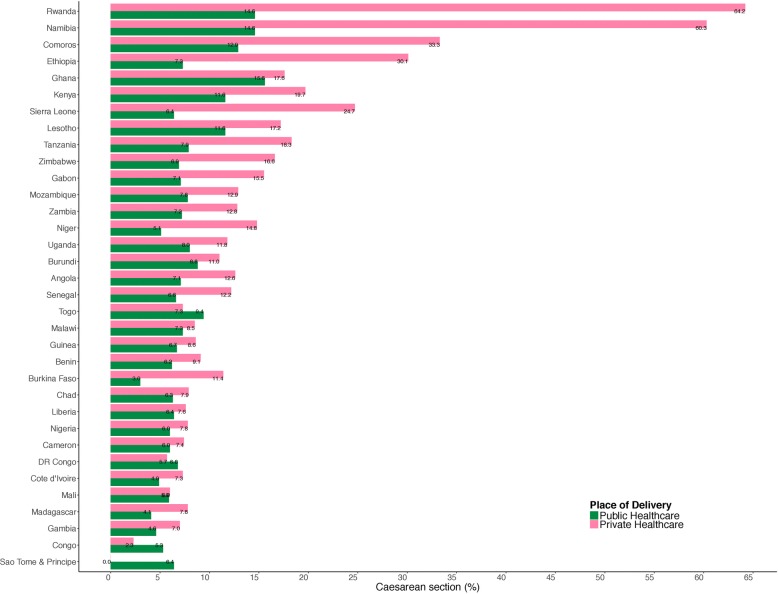
Results: Results showed disparities in the percentage of C-section among women from 34 SSA countries. C-section at public healthcare settings ranged from 3% in Burkina Faso to 15.6% in Ghana. However, in private healthcare settings, C-section ranged from 0% in Sao Tome and Principe to 64.2% in Rwanda. Overall, C-section was 7.9% from public healthcare and 12.3% from private healthcare facilities respectively. In the adjusted regression model; women aged 35-49 had increase in the odds of C-section, while a unit increase in the number of children ever born had 17 and 20% significant reduction in the odds of C-section in public and private healthcare respectively. Assessing public healthcare settings; women from richer/richest households, male and large size children at birth had increase in the odds of C-section, while those from rich neighbourhood had reduction in the odds of C-section. In private healthcare settings, women with high decision making power and multiple births had increase in the odds of C-section, while those who attended ANC visits had significant reduction in the odds of C-section.
Conclusion: The findings from this study would help formulate health policies and implement actions that would improve the outcome of C-section care. Monitoring of emergency obstetric care services is necessary to address issues connected to poor C-section outcomes in resource-constrained settings. Also training of medical personnel including midwives and nurses in emergency obstetric care, ensuring accessibility to life-saving drugs and supplies should be encouraged in health care system.
Keywords: Cesarean section; Delivery; Global health; Maternal health; Sub-Saharan Africa; Vaginal birth.
Conflict of interest statement
Ethics approval for this study was not required since the data is secondary and is available in the public domain. More details regarding DHS data and ethical standards are available at: http://goo.gl/ny8T6X.No consent to publish was needed for this study as we did not use any details, images or videos related to individual participants. In addition data used is available in the public domain.The authors declare that they have no competing interests.
Figures
Similar articles
-
Provision of postpartum care to women giving birth in health facilities in sub-Saharan Africa: A cross-sectional study using Demographic and Health Survey data from 33 countries.PLoS Med. 2019 Oct 23;16(10):e1002943. doi: 10.1371/journal.pmed.1002943. eCollection 2019 Oct. PLoS Med. 2019. PMID: 31644531 Free PMC article.
-
Epidemiology of emergency and elective caesarean section and its association with early neonatal mortality in sub-Saharan African countries.BMJ Open. 2023 Oct 12;13(10):e074995. doi: 10.1136/bmjopen-2023-074995. BMJ Open. 2023. PMID: 37827732 Free PMC article.
-
Determinants of postnatal care utilization in sub-Saharan Africa: a meta and multilevel analysis of data from 36 sub-Saharan countries.Ital J Pediatr. 2020 Nov 27;46(1):175. doi: 10.1186/s13052-020-00944-y. Ital J Pediatr. 2020. PMID: 33246475 Free PMC article.
-
Illuminating Perspectives: Navigating Eye Care Access in Sub-Saharan Africa Through the Social Determinants of Health.Cureus. 2024 Jun 6;16(6):e61841. doi: 10.7759/cureus.61841. eCollection 2024 Jun. Cureus. 2024. PMID: 38975490 Free PMC article. Review.
-
Discharge instructions given to women following delivery by cesarean section in Sub-Saharan Africa: A scoping review.PLOS Glob Public Health. 2022 Apr 22;2(4):e0000318. doi: 10.1371/journal.pgph.0000318. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962191 Free PMC article.
Cited by
-
Late and Persistent Symptoms Suggestive of Surgical Site Infections After Cesarean Section: Results from a Prospective Cohort Study in Rural Rwanda.Surg Infect (Larchmt). 2023 Dec;24(10):916-923. doi: 10.1089/sur.2023.100. Epub 2023 Nov 29. Surg Infect (Larchmt). 2023. PMID: 38032658 Free PMC article.
-
Comparing adverse maternal and perinatal outcomes in primary caesarean delivery during first versus second-stage of labour in Kenya: An institution-based cohort study.PLoS One. 2023 Nov 27;18(11):e0294266. doi: 10.1371/journal.pone.0294266. eCollection 2023. PLoS One. 2023. PMID: 38011095 Free PMC article.
-
Preference and determinants of delivery mode in pregnant women with one cesarean scar: a cross-sectional study in two urban Ugandan public hospitals.BMC Pregnancy Childbirth. 2025 Feb 6;25(1):127. doi: 10.1186/s12884-025-07263-2. BMC Pregnancy Childbirth. 2025. PMID: 39915826 Free PMC article.
-
Multitask Deep Neural Network for the Fully Automatic Measurement of the Angle of Progression.Comput Math Methods Med. 2022 Sep 2;2022:5192338. doi: 10.1155/2022/5192338. eCollection 2022. Comput Math Methods Med. 2022. PMID: 36092792 Free PMC article.
-
Determinants of a high prevalence of cesarean section among women in eastern Uganda.Pan Afr Med J. 2023 Nov 23;46:90. doi: 10.11604/pamj.2023.46.90.38208. eCollection 2023. Pan Afr Med J. 2023. PMID: 38314237 Free PMC article.
References
-
- UN General Assembly, Transforming our world: the 2030 Agenda for Sustainable Development, 21 October 2015, A/RES/70/1. Available at: http://www.refworld.org/docid/57b6e3e44.html. Accessed 3 Mar 2018.
-
- WHO . Trends in Maternal Mortality: 1990 to 2008. Geneva: World Health Organization; 2010.
-
- Lauer JA, Betrán AP, Merialdi M, Wojdyla D. Rates of caesarean section: analysis of global, regional and national estimates. Paediatr Perinatal Epidemiol. 2007;28:98–113. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
