

Maintenance antipsychotic treatment versus discontinuation strategies following remission from first episode psychosis: systematic review
- PMID: 29988997
- PMCID: PMC6034451
- DOI: 10.1192/bjo.2018.17
Maintenance antipsychotic treatment versus discontinuation strategies following remission from first episode psychosis: systematic review
Abstract
Background: Understanding the relative risks of maintenance treatment versus discontinuation of antipsychotics following remission in first episode psychosis (FEP) is an important area of practice.
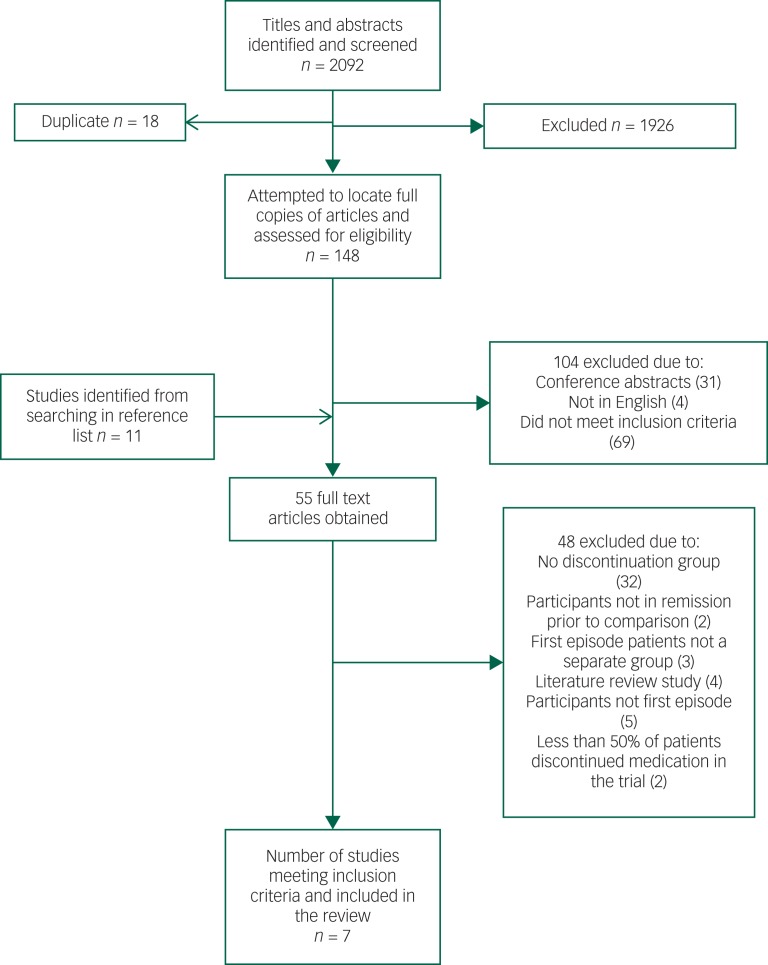
Method: A systematic review and meta-analysis. Prospective experimental studies including a parallel control group were identified to compare maintenance antipsychotic treatment with total discontinuation or medication discontinuation strategies following remission in FEP.
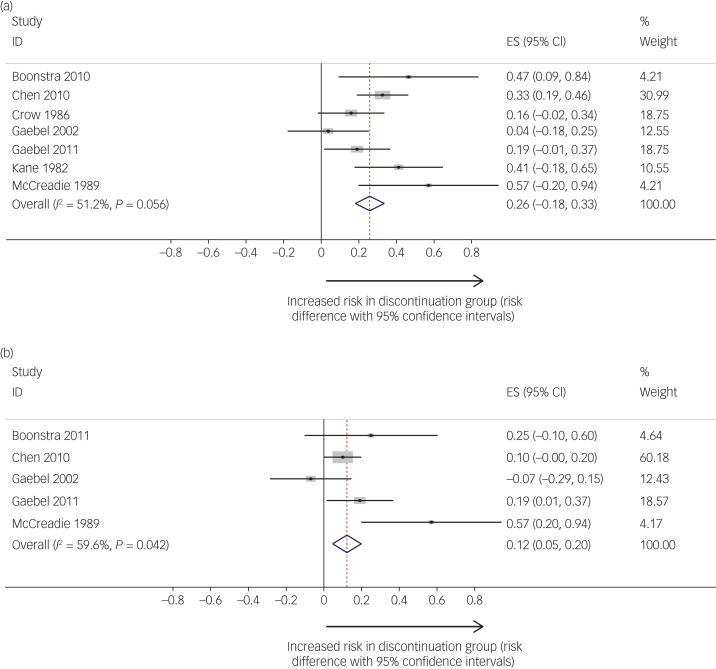
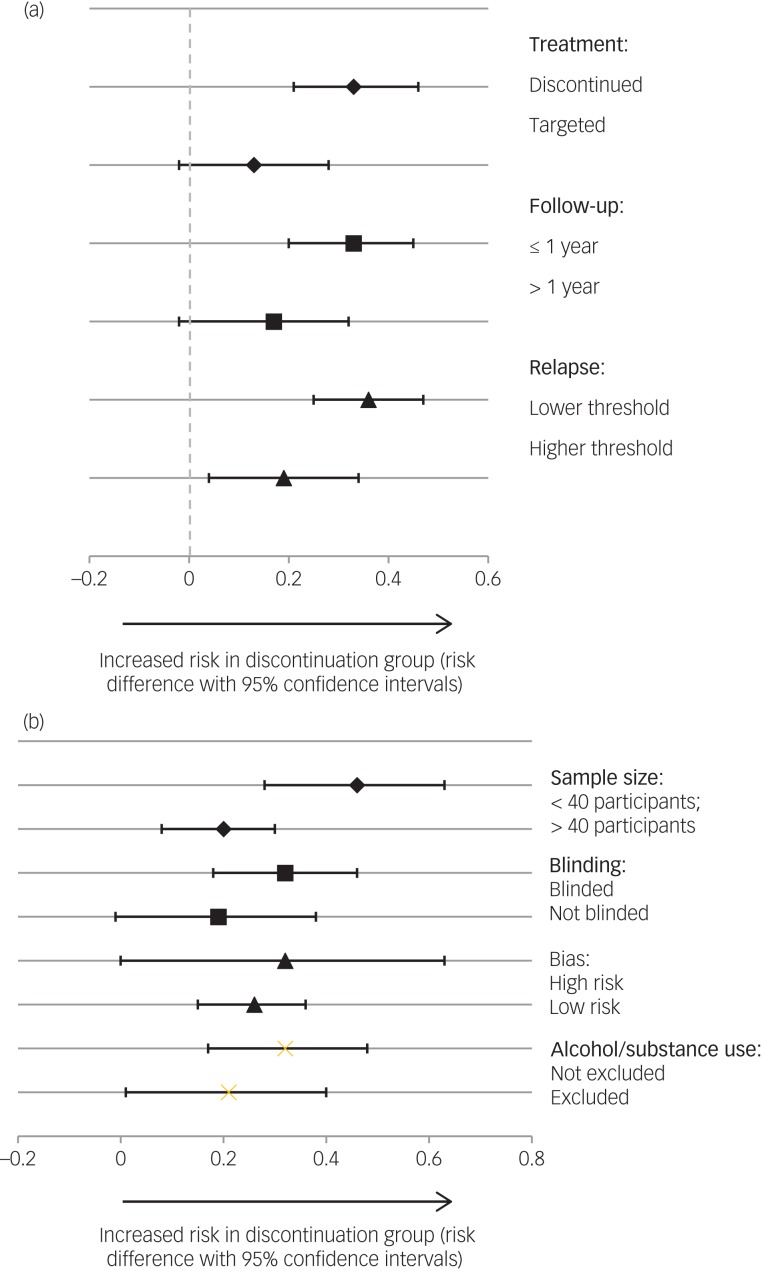
Results: Seven studies were included. Relapse rates were higher in the discontinuation group (53%; 95% CIs: 39%, 68%; N = 290) compared with maintenance treatment group (19%; 95% CIs: 0.05%, 37%; N = 230). In subgroup analyses, risk difference of relapse was lower in studies with a longer follow-up period, a targeted discontinuation strategy, a higher relapse threshold, a larger sample size, and samples with patients excluded for drug or alcohol dependency. Insufficient studies included psychosocial functioning outcomes for a meta-analysis.
Conclusions: There is a higher risk of relapse for those who undergo total or targeted discontinuation strategies compared with maintenance antipsychotics in FEP samples. The effect size is moderate and the risk difference is lower in trials of targeted discontinuation strategies.
Declaration of interest: A.T. has received honoraria and support from Janssen-Cilag and Otsuka Pharmaceuticals for meetings and has been has been an investigator on unrestricted investigator-initiated trials funded by AstraZeneca and Janssen-Cilag. He has also previously held a Pfizer Neurosciences Research Grant. S.M. has received sponsorship from Otsuka and Lundbeck to attend an academic congress and owns shares in GlaxoSmithKline and AstraZeneca. J.H. has attended meetings supported by Sunovion Pharmaceuticals.
Figures
Similar articles
-
Treatment-resistant and multi-therapy-resistant criteria for bipolar depression: consensus definition.Br J Psychiatry. 2019 Jan;214(1):27-35. doi: 10.1192/bjp.2018.257. Epub 2018 Dec 6. Br J Psychiatry. 2019. PMID: 30520709 Free PMC article.
-
Ketamine: stimulating antidepressant treatment?BJPsych Open. 2016 May 11;2(3):e5-e9. doi: 10.1192/bjpo.bp.116.002923. eCollection 2016 May. BJPsych Open. 2016. PMID: 27703782 Free PMC article.
-
Beyond Clinical Remission in First Episode Psychosis: Thoughts on Antipsychotic Maintenance vs. Guided Discontinuation in the Functional Recovery Era.CNS Drugs. 2016 May;30(5):357-68. doi: 10.1007/s40263-016-0331-x. CNS Drugs. 2016. PMID: 27106296 Review.
-
Effect of discontinuation v. maintenance of antipsychotic medication on relapse rates in patients with remitted/stable first-episode psychosis: a meta-analysis.Psychol Med. 2019 Apr;49(5):772-779. doi: 10.1017/S0033291718001393. Epub 2018 Jun 18. Psychol Med. 2019. PMID: 29909790
-
Long-term outcomes of antipsychotic treatment in patients with first-episode schizophrenia: a systematic review.Neuropsychiatr Dis Treat. 2016 Jan 6;12:57-67. doi: 10.2147/NDT.S96392. eCollection 2016. Neuropsychiatr Dis Treat. 2016. PMID: 26792993 Free PMC article. Review.
Cited by
-
To continue or not to continue? Antipsychotic medication maintenance versus dose-reduction/discontinuation in first episode psychosis: HAMLETT, a pragmatic multicenter single-blind randomized controlled trial.Trials. 2020 Feb 7;21(1):147. doi: 10.1186/s13063-019-3822-5. Trials. 2020. PMID: 32033579 Free PMC article.
-
Clinical experiences of guided tapering of antipsychotics for patients with schizophrenia- a case series.BMC Psychiatry. 2024 Mar 29;24(1):240. doi: 10.1186/s12888-024-05699-y. BMC Psychiatry. 2024. PMID: 38553687 Free PMC article.
-
The effects of antipsychotic discontinuation or maintenance on the process of recovery in remitted first-episode psychosis patients - A systematic review and meta-analysis of randomized controlled trials.Eur Psychiatry. 2024 Jan 22;67(1):e13. doi: 10.1192/j.eurpsy.2024.5. Eur Psychiatry. 2024. PMID: 38250810 Free PMC article.
-
Time-dependent effect of antipsychotic discontinuation and dose reduction on social functioning and subjective quality of life-a multilevel meta-analysis.EClinicalMedicine. 2023 Nov 9;65:102291. doi: 10.1016/j.eclinm.2023.102291. eCollection 2023 Nov. EClinicalMedicine. 2023. PMID: 38021372 Free PMC article.
-
A Method for Tapering Antipsychotic Treatment That May Minimize the Risk of Relapse.Schizophr Bull. 2021 Jul 8;47(4):1116-1129. doi: 10.1093/schbul/sbab017. Schizophr Bull. 2021. PMID: 33754644 Free PMC article.
References
-
- Robinson DG, Woerner MG, McMeniman M, Mendelowitz A, Bilder RM. Symptomatic and functional recovery from a first episode of schizophrenia or schizoaffective disorder. Am J Psychiatry 2004; 161: 473–9. - PubMed
-
- Robinson D, Woerner M, Alvir J, Bilder R, Goldman R, Geisler S. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry 1999; 56: 241–7. - PubMed
-
- Kane J. Treatment strategies to prevent relapse and encourage remission. J Clin Psychiatry 2007; 68(suppl 14): 27–30. - PubMed
-
- Lieberman JA, Alvir JM, Koreen A, Geisler S, Chakos M, Sheitman BB, et al. Psychobiologic correlates of treatment response in schizophrenia. Neuropsychopharmacol 1996; 14: 13S–21S. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
