

Prevalence of CKD, Diabetes, and Hypertension in Rural Tanzania
- PMID: 29989050
- PMCID: PMC6035140
- DOI: 10.1016/j.ekir.2018.04.006
Prevalence of CKD, Diabetes, and Hypertension in Rural Tanzania
Abstract
Introduction: Chronic kidney disease (CKD), diabetes, and hypertension play a disproportionate role in the growing public health challenge posed by noncommunicable diseases (NCDs) in East Africa. The impact of these NCDs may pose the greatest challenge in rural areas with limited screening and treatment facilities, although precise prevalence estimates of these conditions in rural Tanzania are lacking.
Methods: The prevalence of CKD, diabetes, and hypertension, were estimated from a probability sample of adults (n = 739) residing in 2 communities within Kisarawe, a rural district of Tanzania. Following consent, participants were studied in their homes. Random point-of-care (POC) measures of glycosylated hemoglobin and blood pressure, were obtained. Serum creatinine, drawn at the POC and measured at Muhimbili National University, was used to calculate estimated glomerular filtration rate with the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.
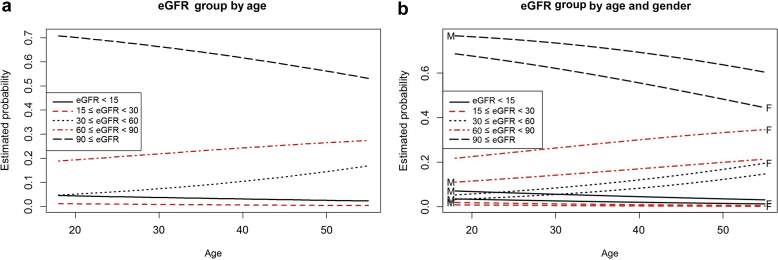
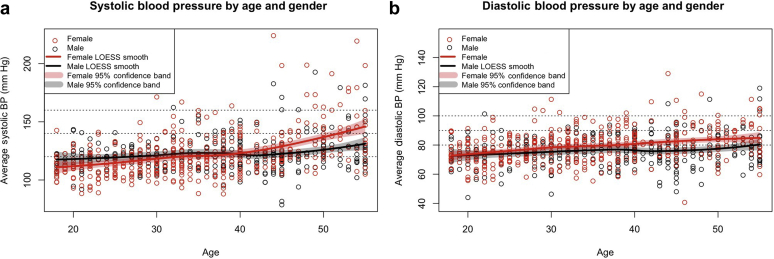
Results: The median age was 35 years (interquartile range 25-45 years). Overall the pooled prevalence for CKD stages III, IV, and V was 12.4% (95% confidence interval [CI] = 10.2-14.8). Surprisingly, the prevalence of CKD stage V (3.0%; 95% CI = 2.1-4.4) was high among the youngest age group (18-36 years). The prevalence estimates for prehypertension and hypertension were 38.0% (95% CI = 34.6-41.5) and 19.9% (95% CI = 17.1-22.9), respectively. The prevalence estimates for prediabetes and diabetes were 25.7% (95% CI = 22.6-29.1) and 14.8% (95% CI = 12.4-17.6), respectively.
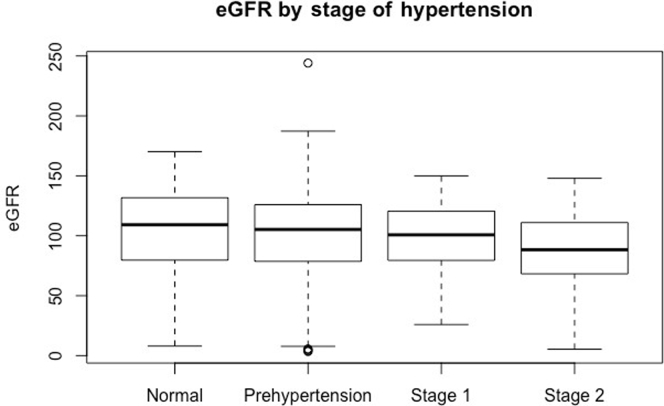
Conclusion: Although this pilot study had a relatively small sample size, the prevalence estimates for CKD, diabetes, and hypertension were higher than we expected based on previous estimates from Tanzania. CKD was not significantly associated with diabetes or hypertension, suggesting the possibility of an alternative causality.
Keywords: Tanzania; diabetes mellitus; hypertension; kidney disease; prevalence.
Figures




References
-
- Kearney P.M., Whelton M., Reynolds K. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–223. - PubMed
-
- Whiting D.R., Guariguata L., Weil C., Shaw J. IDF Diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Practice. 2011;94:311–321. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
