

AAFP Feline Anesthesia Guidelines
- PMID: 29989502
- PMCID: PMC10816483
- DOI: 10.1177/1098612X18781391
AAFP Feline Anesthesia Guidelines
Abstract
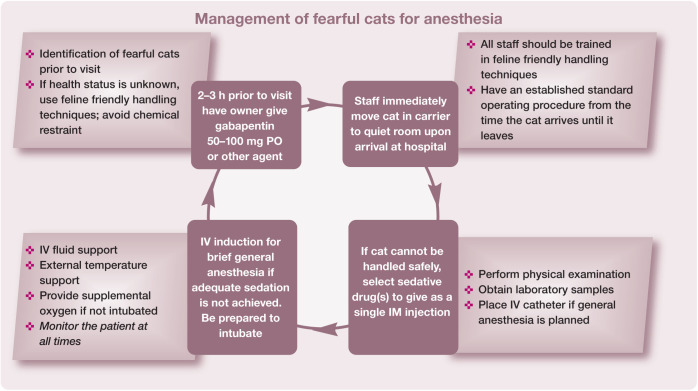
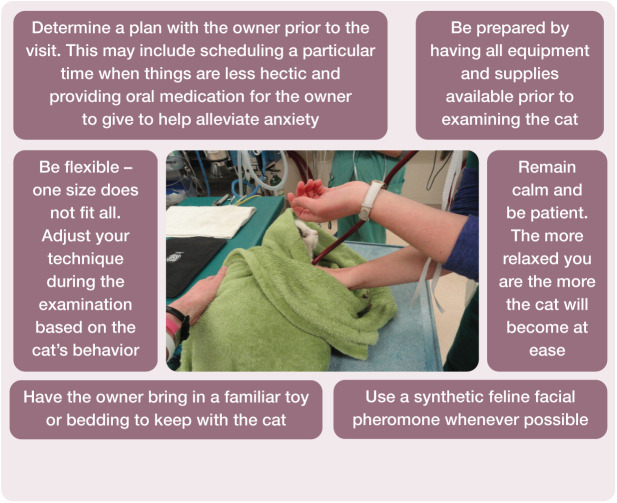
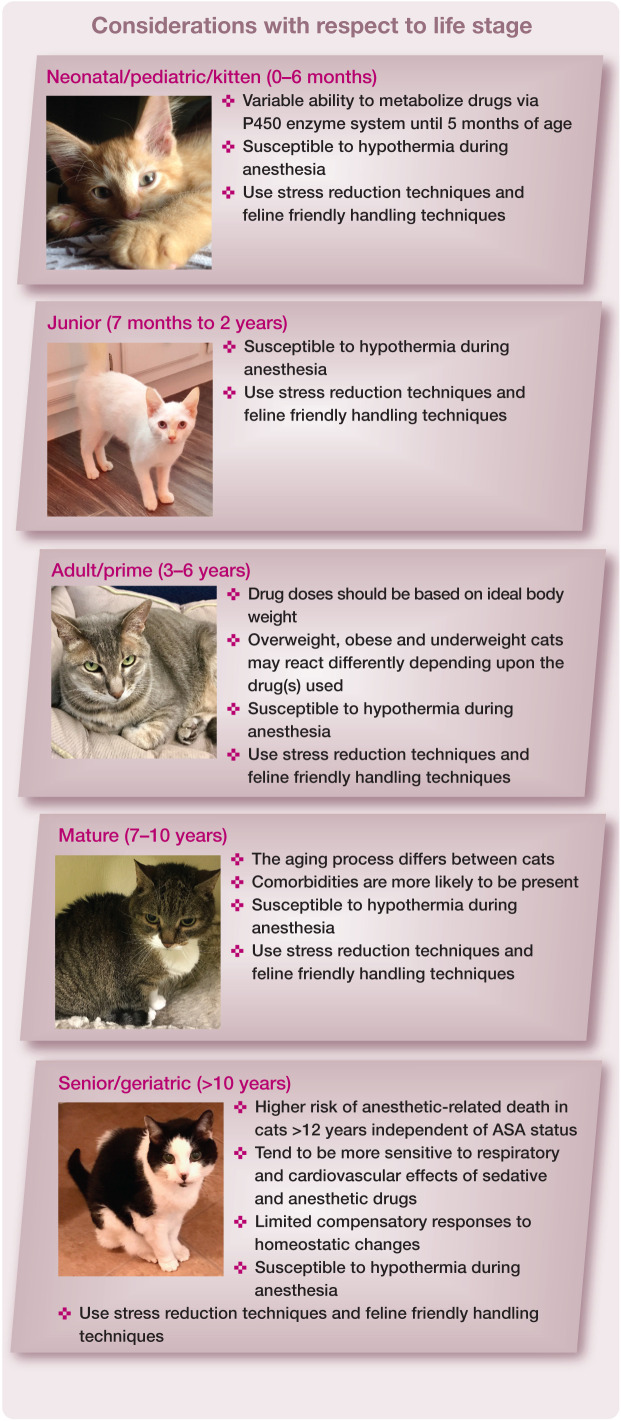
The overarching purpose of the AAFP Anesthesia Guidelines (hereafter referred to as the 'Guidelines') is to make anesthesia and sedation safer for the feline patient. Scope and accessibility: It is noteworthy that these are the first exclusively feline anesthesia guidelines authored by an expert panel, making them particularly useful as an extensively referenced, practical resource for veterinary practice teams. Because much of the key content is presented in tabular or visual format, the Guidelines have a high level of accessibility and convenience that invites regular usage. While the recommendations in the Guidelines focus primarily on client-owned cats, the content is also applicable to community-sourced animals with an unknown medical history.
Keywords: Anesthesia; airway management; anesthetic equipment; comorbidities; monitoring; sedation.
Conflict of interest statement
The Panel members have no conflicts of interest to declare.
Figures








Comment in
-
To sleep, perchance to dream . . . of better anesthesia for our feline patients.J Feline Med Surg. 2018 Jul;20(7):601. doi: 10.1177/1098612X18781387. J Feline Med Surg. 2018. PMID: 29989501 Free PMC article. No abstract available.
References
-
- Dyson DH, Maxie MG, Schnurr D. Morbidity and mortality associated with anesthetic management in small animal veterinary practice in Ontario. J Am Anim Hosp Assoc 1998; 34: 325–335. - PubMed
-
- Brodbelt DC, Pfeiffer DU, Young LE, et al. . Risk factors for anaesthetic-related death in cats: results from the confidential enquiry into perioperative small animal fatalities (CEP-SAF). Br J Anaesth 2007; 99: 617–623. - PubMed
-
- Vogt AH, Rodan I, Brown M, et al. . AAFP–AAHA feline life stage guidelines. J Am Anim Hosp Assoc 2010; 46: 70–85. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
