

Gender and Racial Disparities in Initial Hemodialysis Access and Outcomes in Incident End-Stage Renal Disease Patients
- PMID: 29990994
- PMCID: PMC6159828
- DOI: 10.1159/000490624
Gender and Racial Disparities in Initial Hemodialysis Access and Outcomes in Incident End-Stage Renal Disease Patients
Abstract
Background: Arteriovenous (AV) access confers survival benefits over central venous catheters (CVC) in hemodialysis patients. Although chronic kidney disease disproportionately affects women and racial minorities, disparities in the -utilization of hemodialysis access across Asians, Native Americans, Hispanics, blacks, and whites among males and females after accounting for pre-dialysis health are not well studied.
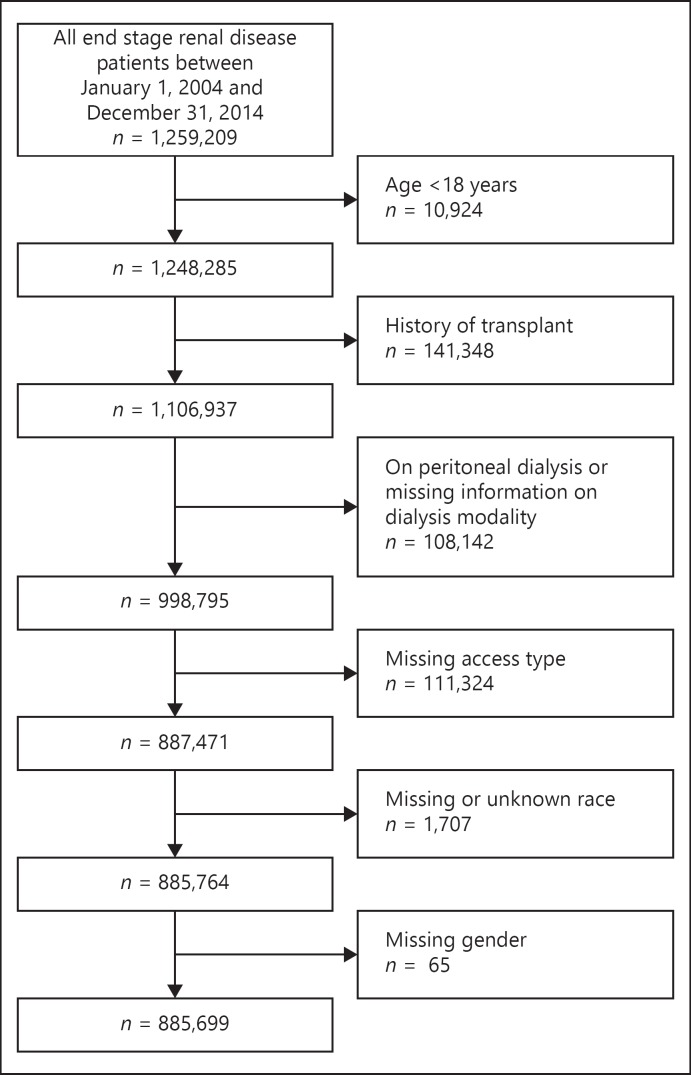
Methods: We evaluated 885,699 patients with end-stage renal disease who initiated hemodialysis between January 1, 2004 and December 31, 2014 using the US Renal Data System. Multivariable logistic regression models -adjusted for pre-dialysis health were used to test the associations between gender and race on type of vascular access (AV access vs. CVC, and AV fistula vs. AV graft) at hemodialysis initiation as primary outcome, and on 1-year mortality as a secondary outcome.
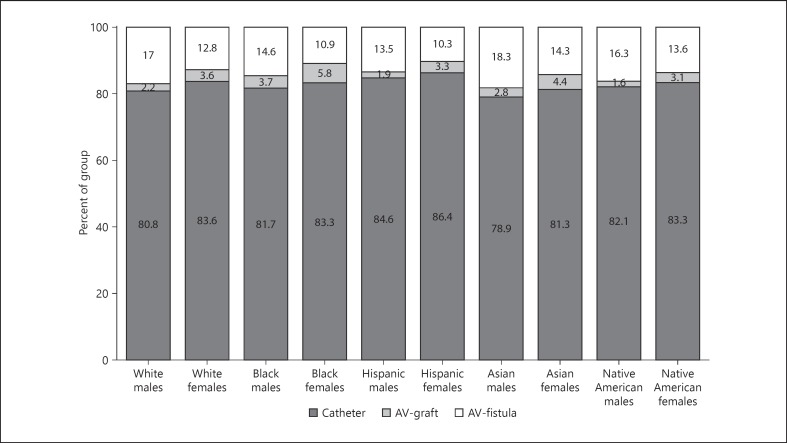
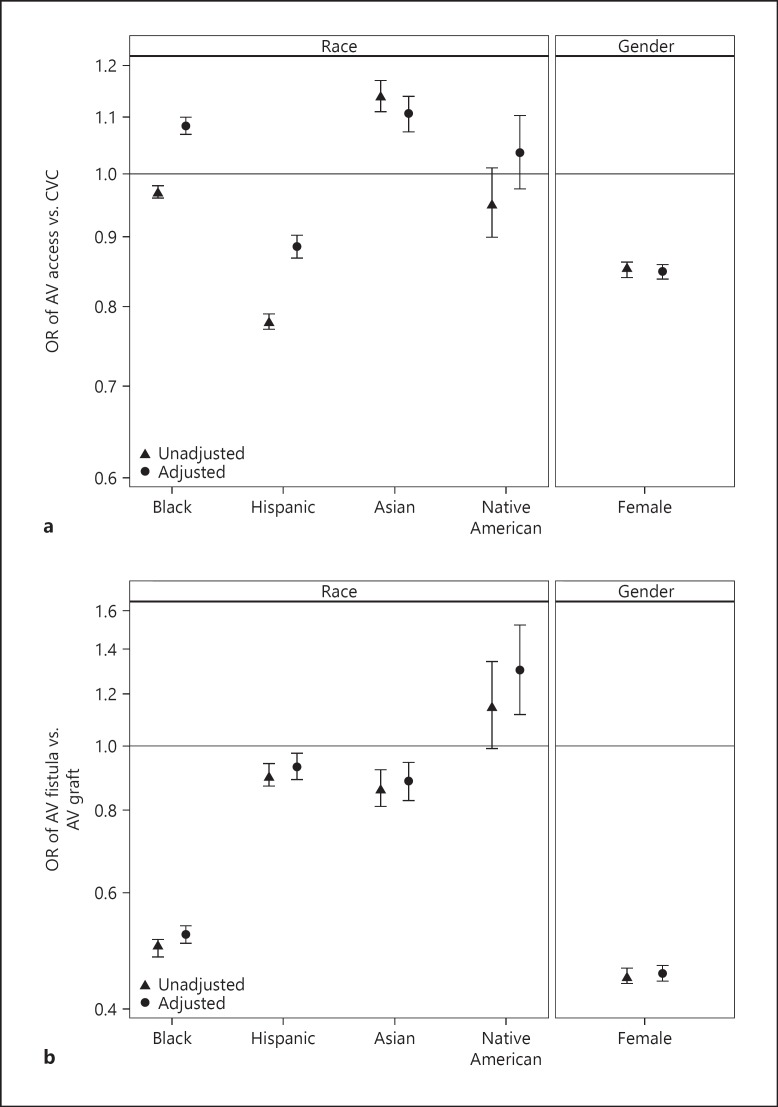
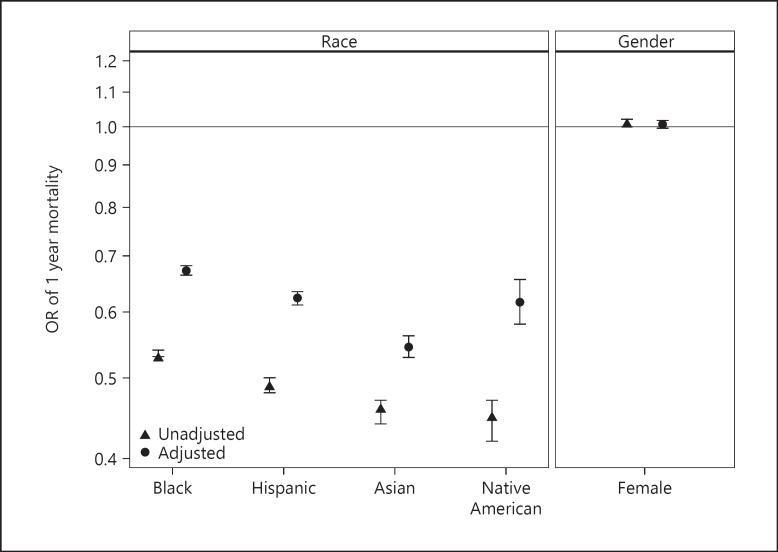
Results: Mean age was 65 ± 14 years. Females were less likely to use AV access for hemodialysis initiation than were males (OR 0.85; 95% CI 0.84-0.86). Compared to whites, adjusted odds of AV access for hemodialysis initiation were higher in blacks (OR 1.08; 95% CI 1.07-1.70), Asians (OR 1.11; 95% CI 1.07-1.14); and lower in Hispanics (OR 0.89; 95% CI 0.87-0.90). There was no -significant difference in mortality between males and females. Compared to whites, 1-year adjusted mortality was lower in Asians (OR 0.55; 95% CI 0.53-0.56), blacks (OR 0.67; 95% CI 0.66-0.68), Hispanics (OR 0.62; 95% CI 0.61-0.63), and Native Americans (OR 0.62; 95% CI 0.58-0.66).
Conclusion: Females had lower odds of using AV access than do males for hemodialysis initiation. As compared to whites, blacks and Asians were more likely, and Hispanics were less likely to use AV access for first outpatient hemodialysis. Further investigation of biological and process of care factors may help in developing ways to reduce these disparities.
Keywords: Disparities; Gender; Hemodialysis; Mortality; Race; Vascular access.
The Author(s). Published by S. Karger AG, Basel.
Figures
Comment in
-
Vascular Access Differences in Men and Women: Time to Solve the Problem?Am J Nephrol. 2018;48(1):1-3. doi: 10.1159/000490625. Epub 2018 Jul 10. Am J Nephrol. 2018. PMID: 29990962 No abstract available.
References
-
- U.S. Renal Data System Researcher's Guide to the USRDS Database. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda. 2015
-
- Hecking M, Bieber BA, Ethier J, Kautzky-Willer A, Sunder-Plassmann G, Saemann MD, Ramirez SP, Gillespie BW, Pisoni RL, Robinson BM, Port FK. Sex-specific differences in hemodialysis prevalence and practices and the male-to-female mortality rate: the Dialysis Outcomes and Practice Patterns Study (DOPPS) PLoS Med. 2014;11:e1001750. - PMC - PubMed
-
- Kalantar-Zadeh K, Block G, Humphreys MH, Kopple JD. Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int. 2003;63:793–808. - PubMed
-
- Agodoa L, Eggers P. Racial and ethnic disparities in end-stage kidney failure-survival paradoxes in African-Americans. Semin Dial. 2007;20:577–585. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
