

Craniofacial Phenotyping in Chinese and Caucasian Patients With Sleep Apnea: Influence of Ethnicity and Sex
- PMID: 29991423
- PMCID: PMC6040806
- DOI: 10.5664/jcsm.7212
Craniofacial Phenotyping in Chinese and Caucasian Patients With Sleep Apnea: Influence of Ethnicity and Sex
Abstract
Study objectives: Craniofacial abnormalities are a risk factor for obstructive sleep apnea (OSA). We have previously shown that phenotypic information derived from craniofacial photographs predict OSA in sleep clinic populations. However, there are likely ethnic and sex differences in craniofacial phenotypes related to OSA. We aimed to assess the use of craniofacial photography to identify interactions between OSA, ethnicity, and sex in craniofacial phenotype.
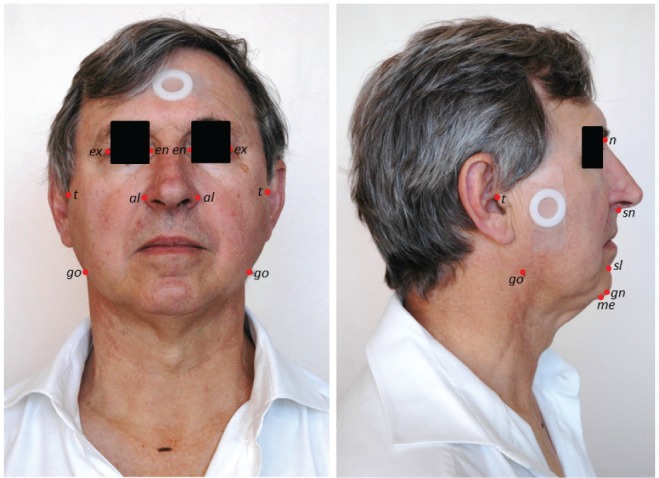
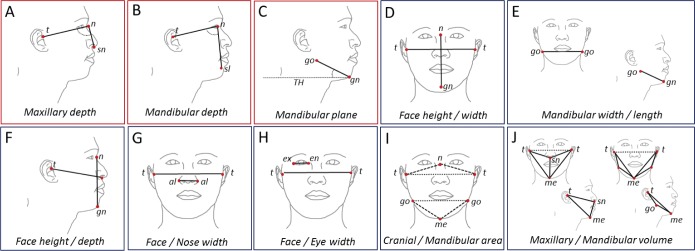
Methods: Frontal and profile craniofacial photographs were analyzed from two sleep clinic populations of different ethnicity (Hong Kong Chinese, Australian Caucasians). OSA was defined as apnea-hypopnea index (AHI) > 10 events/h. Ten craniofacial measurements (three angles relating to jaw position and seven ratios describing proportions of the face) were examined for interactions between OSA status and sex or ethnicity) using factorial analysis of variance.
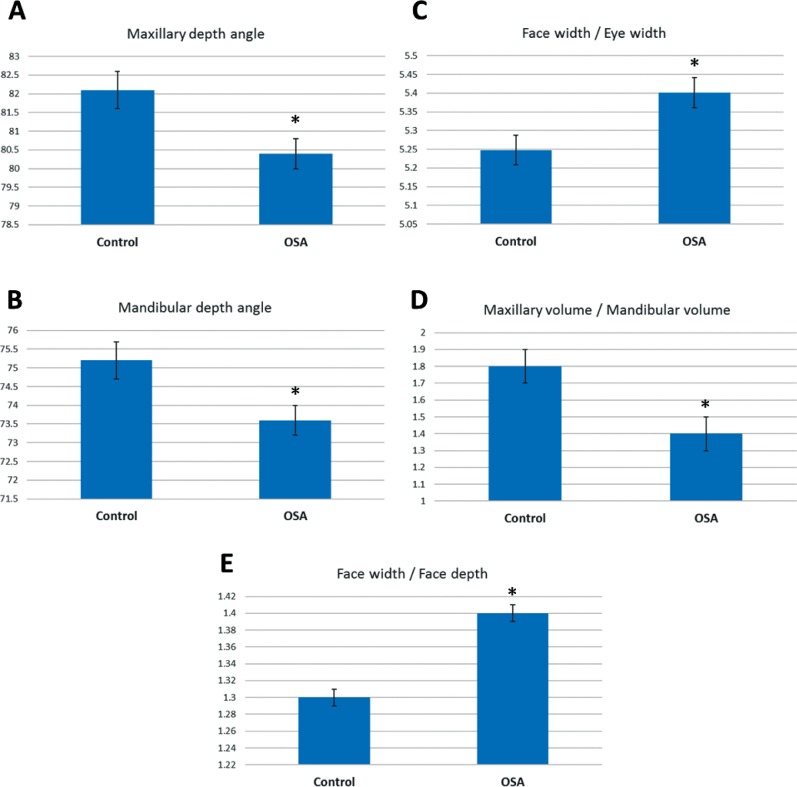
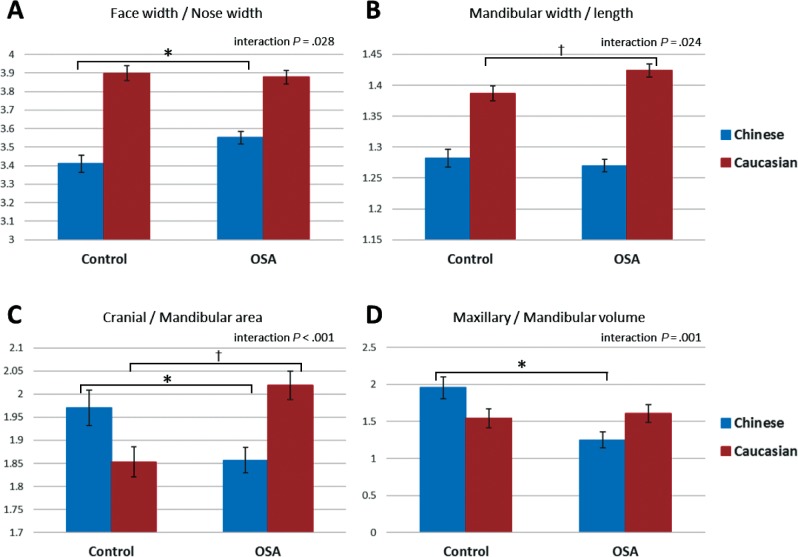
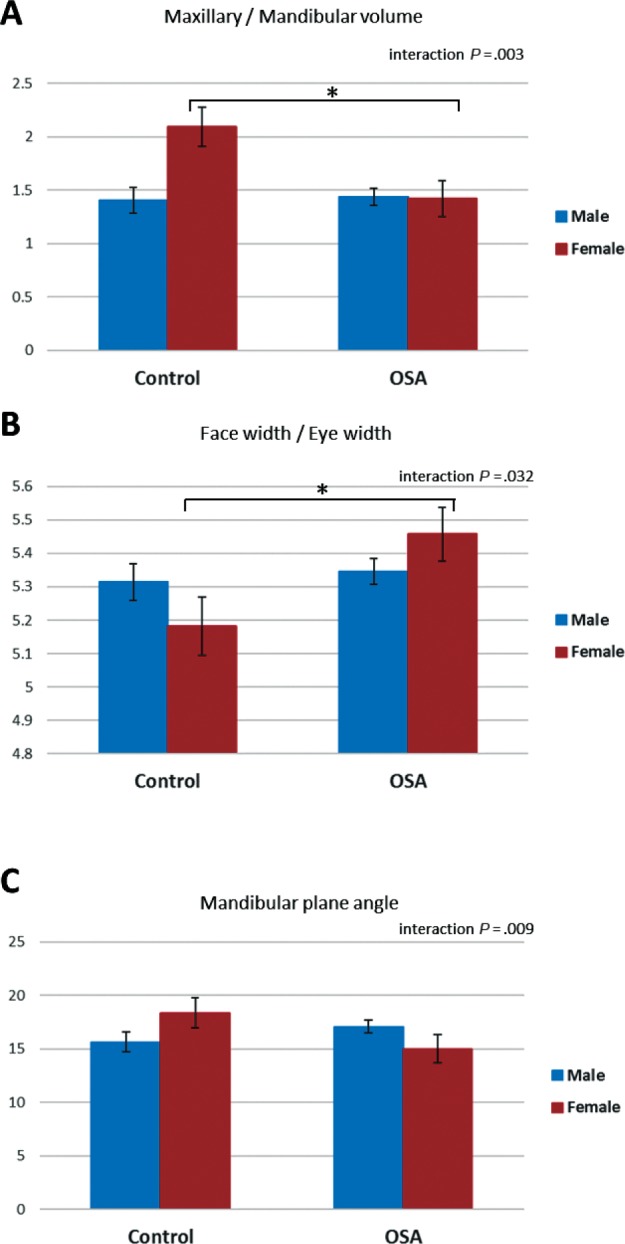
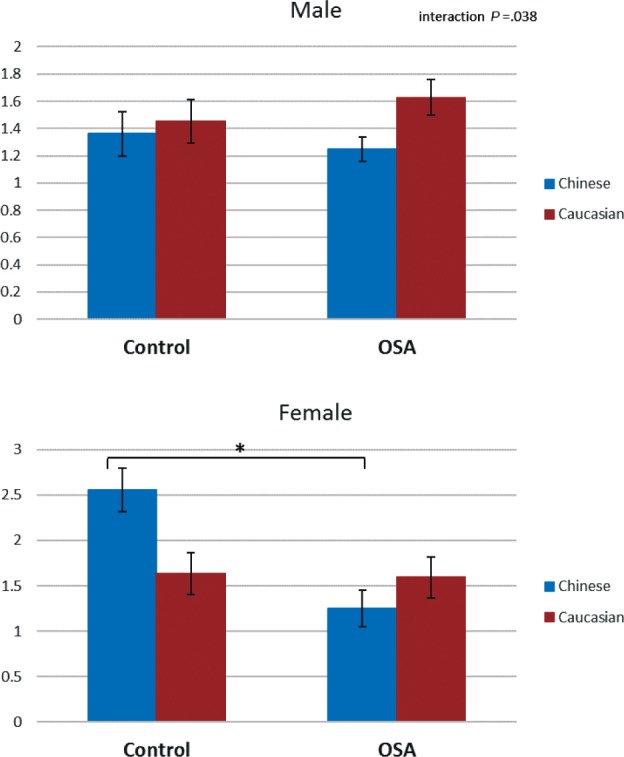
Results: A total of 363 subjects (25% female) were included (n = 200 Chinese, n = 163 Caucasian), of which 33% were controls. There were two-way interactions for OSA with both sex (mandibular plane angle [F = 7.0, P = .009], face / eye width ratio [F = 4.7, P = .032], maxillary / mandibular volume ratio [F = 9.2, P = .003]) and ethnicity (face / nose width ratio [F = 4.0, P = .045], mandibular width / length ratio [F = 5.1, P = .024], maxillary / mandibular volume ratio [F = 11.0, P = .001]).
Conclusions: We provide evidence of ethnic and sex differences in facial phenotype related to OSA. Furthermore, we demonstrate that craniofacial photography can be used as a phenotypic tool to assess these differences and allow investigation of OSA phenotypes in large samples. This has relevance to personalizing OSA recognition strategies across different populations.
Keywords: craniofacial; ethnicity; facial phenotype; obstructive sleep apnea; photogrammetry; sex.
© 2018 American Academy of Sleep Medicine.
Figures
References
-
- Neelapu BC, Kharbanda OP, Sardana HK, et al. Craniofacial and upper airway morphology in adult obstructive sleep apnea patients: a systematic review and meta-analysis of cephalometric studies. Sleep Med Rev. 2017;31:79–90. - PubMed
-
- Schwab RJ, Pasirstein M, Pierson R, et al. Identification of upper airway anatomic risk factors for obstructive sleep apnea with volumetric magnetic resonance imaging. Am J Respir Crit Care Med. 2003;168(5):522–530. - PubMed
-
- Watanabe T, Isono S, Tanaka A, Tanzawa H, Nishino T. Contribution of body habitus and craniofacial characteristics to segmental closing pressures of the passive pharynx in patients with sleep-disordered breathing. Am J Respir Crit Care Med. 2002;165(2):260–265. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
