

A retrospective study of the clinical features of new syphilis infections in an HIV-positive cohort in Alberta, Canada
- PMID: 29991630
- PMCID: PMC6082489
- DOI: 10.1136/bmjopen-2018-021544
A retrospective study of the clinical features of new syphilis infections in an HIV-positive cohort in Alberta, Canada
Abstract
Objectives: Syphilis is a global health concern with an estimated 12 million infections occurring annually. Due to the increasing rates of new syphilis infections being reported in patients infected with HIV, and their higher risk for atypical and severe presentations, periodic screening has been recommended as a routine component of HIV care. We aimed to characterise incident syphilis presentation, serological features and treatment response in a well-defined, HIV-infected population over 11 years.
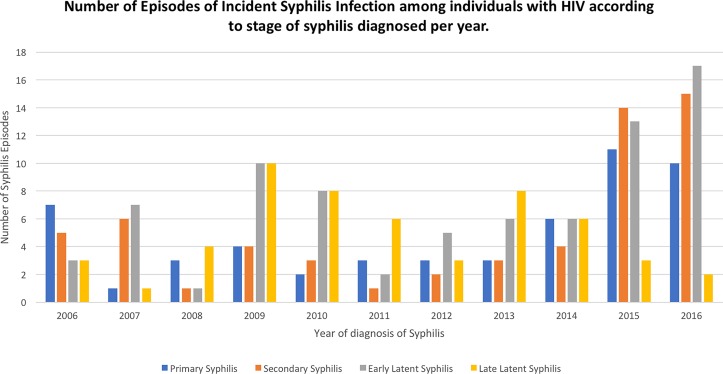
Methods: Since 2006, as routine practice of both the Southern Alberta Clinic and Calgary STI programmes, syphilis screening has accompanied HIV viral load measures every 4 months. All records of patients who, while in HIV care, either converted from being syphilis seronegative to a confirmed seropositive or were reinfected as evidenced by a fourfold increase in rapid plasma reagin (RPR) after past successful treatment, were reviewed.
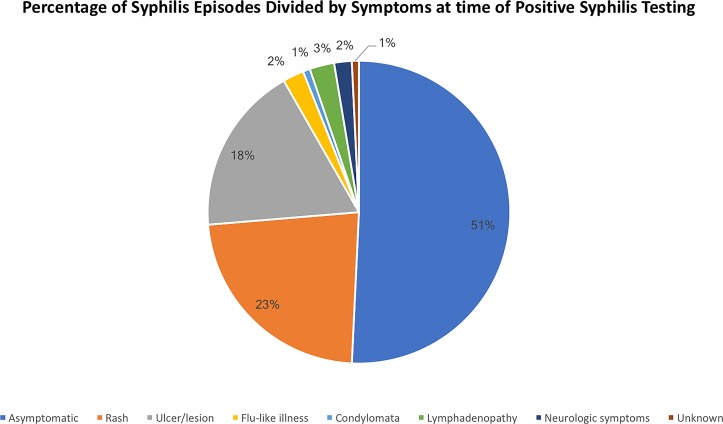
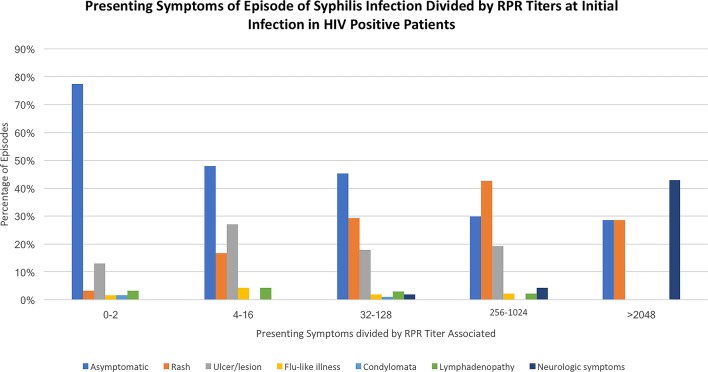
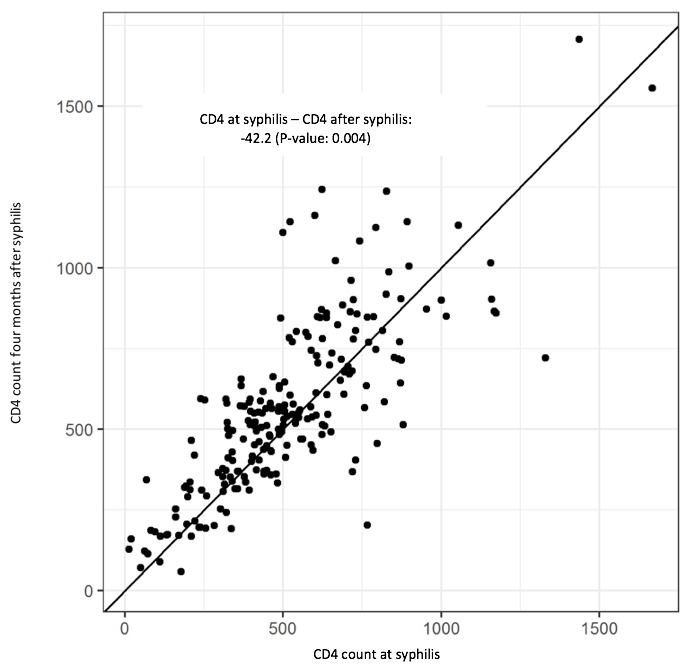
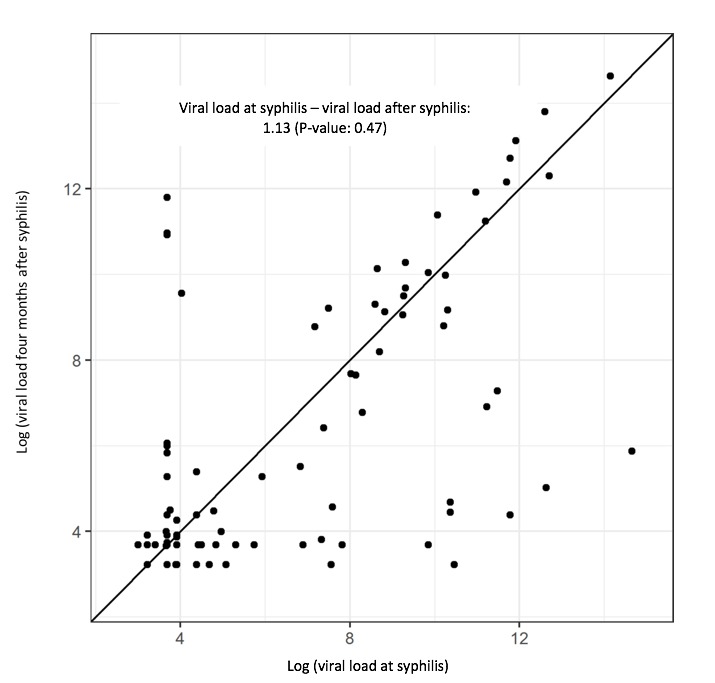
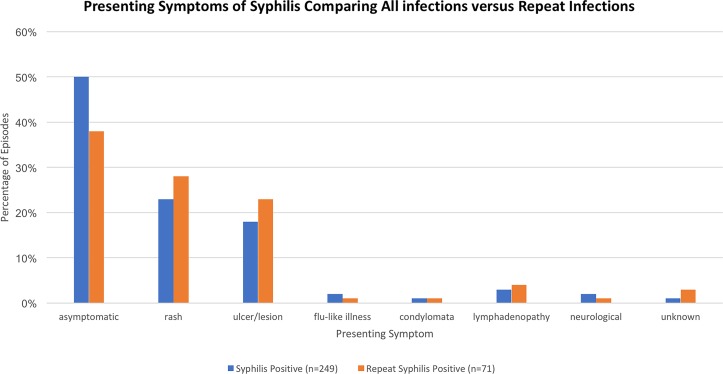
Results: We identified 249 incident syphilis infections in 194 different individuals infected with HIV; 72% were initial infections whereas 28% were reinfections. Half (50.8%) of the infections were asymptomatic and identified only by routine screening. Symptomatic syphilis was more common when RPR titres were higher (p=0.03). In patients with recurrent syphilis infection, a trend was noted favouring symptomatic presentation (62%, p=0.07). All 10 patients with central nervous system (CNS) syphilis involvement presented with an RPR titre ≥1:32. Following syphilis infection, a decline of 42 cells/mm3 in CD4 (p=0.004) was found, but no significant changes in viral load occurred. No association was found with the stage of syphilis or symptoms at presentation and antiretroviral therapy use, CD4 count or virological suppression.
Conclusion: Routine screening of our HIV-infected population identified many asymptomatic syphilis infections. The interaction of HIV and syphilis infection appears to be bidirectional with effects noted on both HIV and syphilis clinical and serological markers.
Keywords: epidemiology; public health.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization. Global incidence and prevalence of selected curable sexually transmitted infections – 2008, 2012. http://www.who.int/reproductivehealth/publications/rtis/stisestimates/en/ (accessed: 6 Dec 2017).
-
- v Mabior R. 2012 SCC 47. 2012. https://scc-csc.lexum.com/scc-csc/scc-csc/en/item/10008/index.do
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous