

Pneumoconiosis in a polytetrafluoroethylene (PTFE) spray worker: a case report with an occupational hygiene study
- PMID: 29992029
- PMCID: PMC5987387
- DOI: 10.1186/s40557-018-0248-6
Pneumoconiosis in a polytetrafluoroethylene (PTFE) spray worker: a case report with an occupational hygiene study
Abstract
Background: Using analysis of air samples from the workplace, we report on one case of pneumoconiosis in an individual who has been working in a polytetrafluoroethylene (PTFE) spraying process for 28 years.
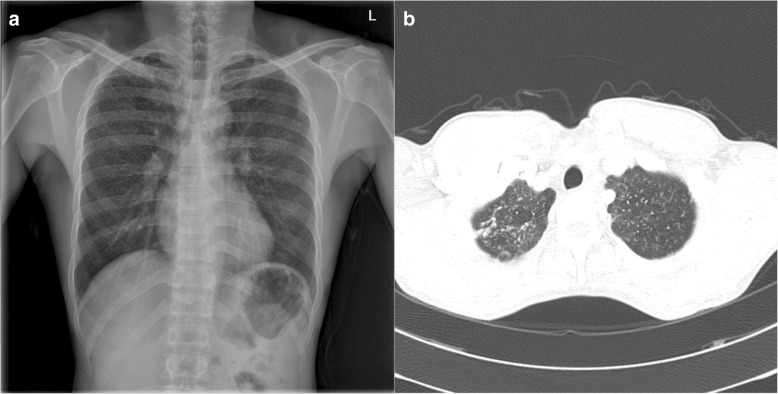
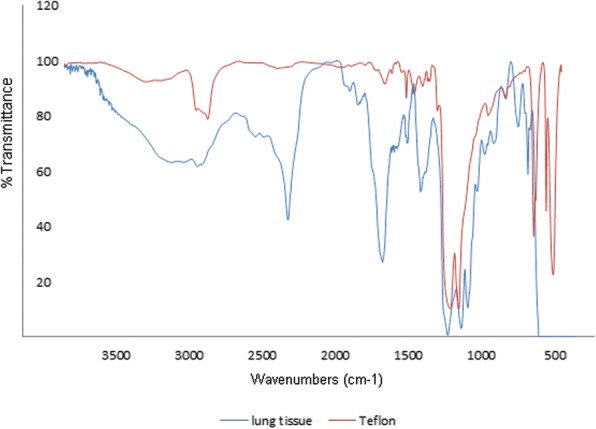
Case presentation: The patient was diagnosed with granulomatous lung disease caused by PTFE using computed tomography (CT), lung biopsy and electron microscopy. To assess the qualitative and quantitative exposure to PTFE in workplace, Fourier transform infrared spectroscopy (FT-IR), energy-dispersive X-ray spectroscopy (EDX) and thermogravimetric analysis (TGA) were performed on air samples from the workplace. The presence of PTFE particles was confirmed, and the airborne concentration of PTFE was estimated to be 0.75 mg/m3.
Conclusions: This case demonstrates that long-term exposure to PTFE spraying can cause granulomatous lung lesions such as pneumoconiosis; such lesions appear to be caused not by the degradation products of PTFE from high temperatures but by spraying the particles of PTFE. Along with air-sampling analysis, we suggest monitoring the concentration of airborne PTFE particles related to chronic lung disease.
Keywords: Occupational diseases; Pneumoconiosis; Polytetrafluoroethylene.
Conflict of interest statement
This study was approved by Keimyung university Dongsan medical center institutional review board. The number of approval is 2016–02–024-008.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Teng H. Overview of the development of the fluoropolymer industry. Appl Sci. 2012;2(2):496–512. doi: 10.3390/app2020496. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
