

Giant Adrenal Myelolipoma in a Patient without Endocrine Disorder: A Case Report and a Review of the Literature
- PMID: 29992078
- PMCID: PMC6016169
- DOI: 10.1155/2018/4854368
Giant Adrenal Myelolipoma in a Patient without Endocrine Disorder: A Case Report and a Review of the Literature
Abstract
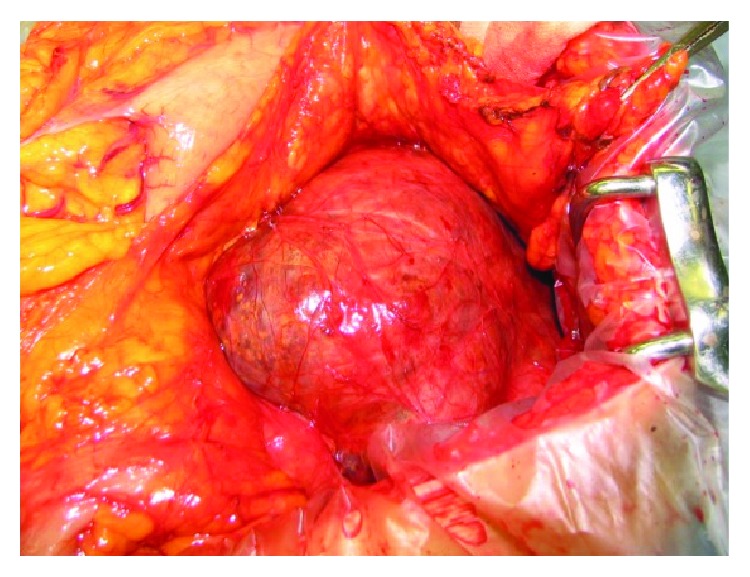
We herein present a surgically treated case of huge adrenal myelolipoma. A 62-year-old woman presented to our surgical outpatient clinic with a retroperitoneal tumor. A clinical examination revealed an elastic soft, smooth-surfaced, painless, child-head-sized tumor with poor mobility, which was located in the left upper abdomen. Computed tomography (CT) and magnetic resonance imaging (MRI) of the abdomen revealed an uneven tumor surrounding the stomach, spleen, pancreas, and left kidney, which was 20 × 18 × 10 cm in size. The retroperitoneal tumor was resected. The tumor was attached to the surrounding organs, including the pancreas, spleen, and left kidney, but had not directly invaded these organs. The tumor was yellow and elastic soft and covered with a thin film. The origin of the tumor was suggested to be the left adrenal gland. The weight of the excised tumor was 1500 g. The histopathological diagnosis was adrenal myelolipoma. The patient had an uneventful recovery and was discharged from the hospital on the thirteenth day after the operation. She has been followed up in our outpatient clinic.
Figures




Similar articles
-
[Bilateral adrenal myelolipoma: a case report].Hinyokika Kiyo. 1994 Aug;40(8):695-8. Hinyokika Kiyo. 1994. PMID: 7942367 Japanese.
-
Giant adrenal myelolipoma with hemorrhage masquerading as retroperitoneal sarcoma.J Midlife Health. 2012 Jan;3(1):42-4. doi: 10.4103/0976-7800.98818. J Midlife Health. 2012. PMID: 22923980 Free PMC article.
-
[A case of myelolipoma arising from accessory adrenal gland].Hinyokika Kiyo. 1993 Jan;39(1):37-40. Hinyokika Kiyo. 1993. PMID: 8460584 Japanese.
-
[Myelolipoma of the adrenal gland presenting as upper abdominal symptoms: a case report].Hinyokika Kiyo. 2003 Nov;49(11):667-70. Hinyokika Kiyo. 2003. PMID: 14719455 Review. Japanese.
-
[A case of a giant adrenal myelolipoma in a man with spinal cord injury].Hinyokika Kiyo. 2007 Jun;53(6):387-91. Hinyokika Kiyo. 2007. PMID: 17628936 Review. Japanese.
Cited by
-
Giant symptomatic adrenal myelolipoma: A case report.Ann Med Surg (Lond). 2022 Feb 9;75:103333. doi: 10.1016/j.amsu.2022.103333. eCollection 2022 Mar. Ann Med Surg (Lond). 2022. PMID: 35198182 Free PMC article.
-
Adrenal Incidentaloma: Challenges in Diagnosing Adrenal Myelolipoma.J Investig Med High Impact Case Rep. 2019 Jan-Dec;7:2324709619870311. doi: 10.1177/2324709619870311. J Investig Med High Impact Case Rep. 2019. PMID: 31434506 Free PMC article.
-
Management of bilateral adrenal myelolipoma without endocrine disorder: About a rare case report.Urol Case Rep. 2021 Jun 15;39:101755. doi: 10.1016/j.eucr.2021.101755. eCollection 2021 Nov. Urol Case Rep. 2021. PMID: 34221899 Free PMC article.
-
A Rare Case of Catecholamine-Secreting Adrenal Myelolipoma.J ASEAN Fed Endocr Soc. 2025 May;40(1):104-107. doi: 10.15605/jafes.040.01.15. Epub 2025 Apr 25. J ASEAN Fed Endocr Soc. 2025. PMID: 40416490 Free PMC article.
-
A Case Report and Literature Review of Adrenal Myelolipoma.Cureus. 2023 Aug 9;15(8):e43240. doi: 10.7759/cureus.43240. eCollection 2023 Aug. Cureus. 2023. PMID: 37692624 Free PMC article.
References
-
- Olsson C. A., Krane R. J., Klugo R. C., Selikowitz S. M. Adrenal myelolipoma. Surgery. 1973;73(5):665–670. - PubMed
-
- Wagnerová H., Lazúrová I., Bober J., Sokol L., Zachar M. Adrenal myelolipoma. 6 cases and a review of the literature. Neoplasma. 2004;51(4):300–305. - PubMed
-
- Daneshmand S., Quek M. L. Adrenal myelolipoma: diagnosis and management. Urology Journal. 2006;3(2):71–74. - PubMed
-
- Nermoen I., Rørvik J., Holmedal S. H., et al. High frequency of adrenal myelolipomas and testicular adrenal rest tumours in adult Norwegian patients with classical congenital adrenal hyperplasia because of 21-hydroxylase deficiency. Clinical Endocrinology. 2011;75(6):753–759. doi: 10.1111/j.1365-2265.2011.04151.x. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
