

Reshaping Movement Distributions With Limit-Push Robotic Training
- PMID: 29994313
- PMCID: PMC8780733
- DOI: 10.1109/TNSRE.2018.2839565
Reshaping Movement Distributions With Limit-Push Robotic Training
Abstract
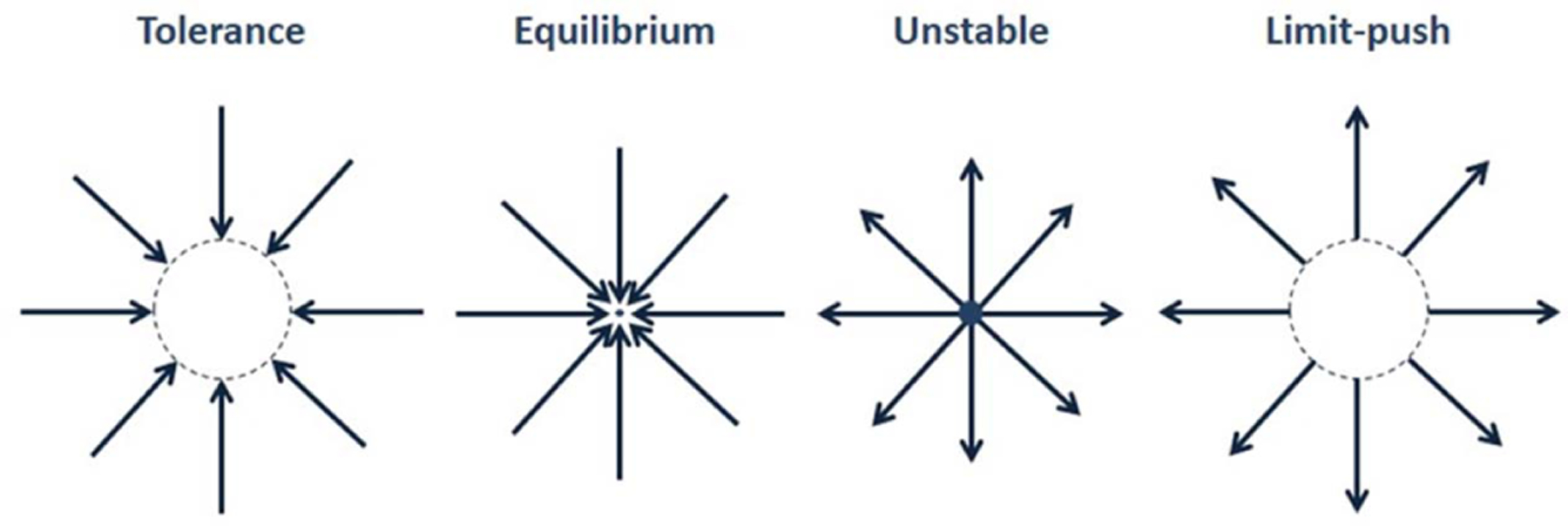
High-cost situations need to be avoided. However, occasionally, cost may only be learned by experience. Here, we tested whether an artificially induced unstable and invisible high-cost region, a "limit-push" force field, might reshape people's motion distributions. Healthy and neurologically impaired (chronic stroke) populations attempted 600 interceptions of a projectile while holding a robot handle that could render forces to the hand. The "limit-push," in the middle of the study, pushed the hand outward unless the hand stayed within a box-shaped region. Both healthy and some stroke survivors adapted through selection of safer actions, avoiding the high-cost regions (outside the box); they stayed more inside and even kept a greater distance from the box's boundaries. This was supported by other measures that showed subjects distributed their hand movements within the box more uniformly. These effects lasted a very short time after returning to the no-force condition. Although most robotic teaching approaches focus on shifting the mean, this limit-push treatment demonstrates how both mean and variance might be reshaped in motor training and neurorehabilitation.
Figures








References
-
- Hausdorff JM, Rios DA, and Edelberg HK, “Gait variability and fall risk in community-living older adults: A 1-year prospective study,” Arch. Phys. Med. Rehabil, vol. 82, no. 8, pp. 1050–1056, Aug. 2001. - PubMed
-
- Armand M, Huissoon JP, and Patla AE, “Stepping over obstacles during locomotion: Insights from multiobjective optimization on set of input parameters,” IEEE Trans. Rehabil. Eng, vol. 6, no. 1, pp. 43–52, Mar. 1998. - PubMed
-
- Branton P, “A field study of repetitive manual work in relation to accidents at the work place,” Int. J. Prod. Res, vol. 8, no. 2, pp. 93–107, 1970.
-
- Kamper DG, McKenna-Cole AN, Kahn LE, and Reinkensmeyer DJ, “Alterations in reaching after stroke and their relation to movement direction and impairment severity,” Arch. Phys. Med. Rehabil, vol. 83, pp. 702–707, May 2002. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
