

Accounting for Label Uncertainty in Machine Learning for Detection of Acute Respiratory Distress Syndrome
- PMID: 29994592
- PMCID: PMC6351314
- DOI: 10.1109/JBHI.2018.2810820
Accounting for Label Uncertainty in Machine Learning for Detection of Acute Respiratory Distress Syndrome
Abstract
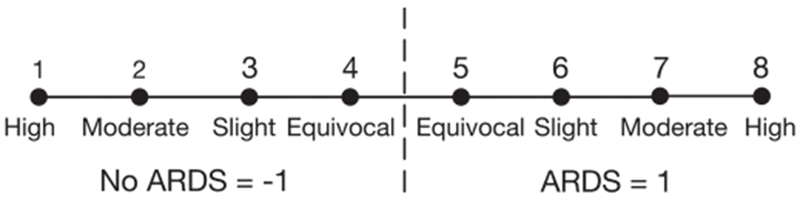
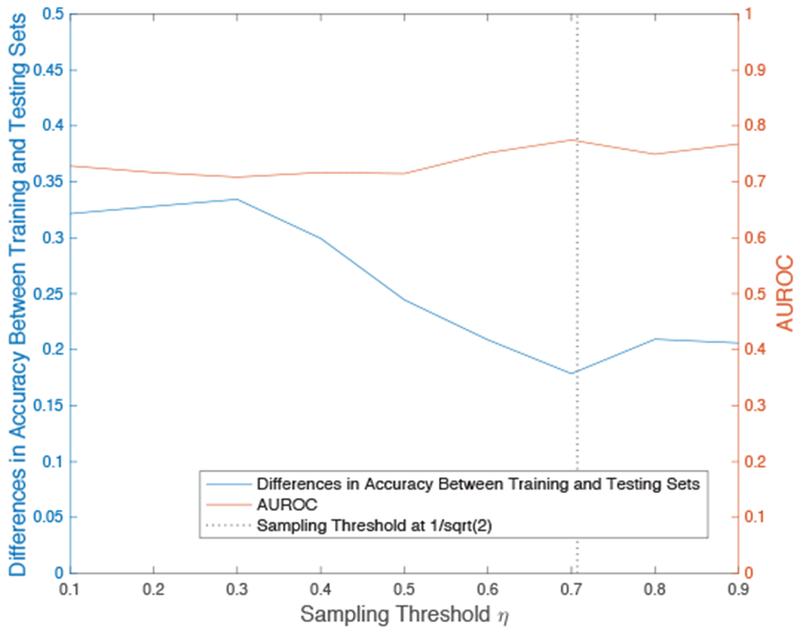
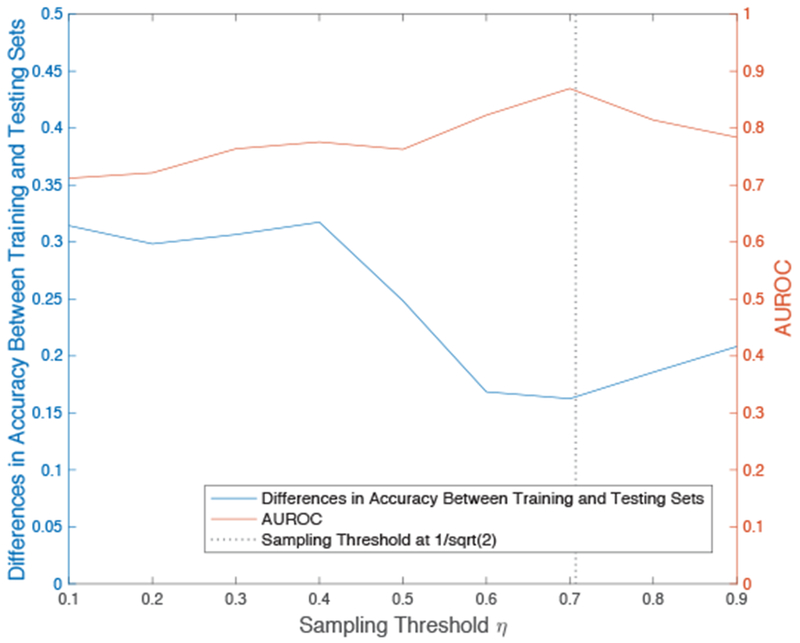
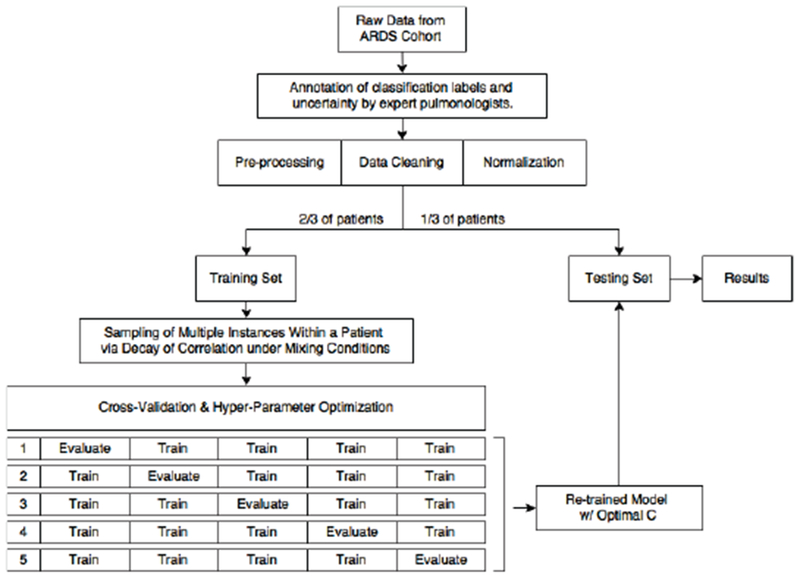
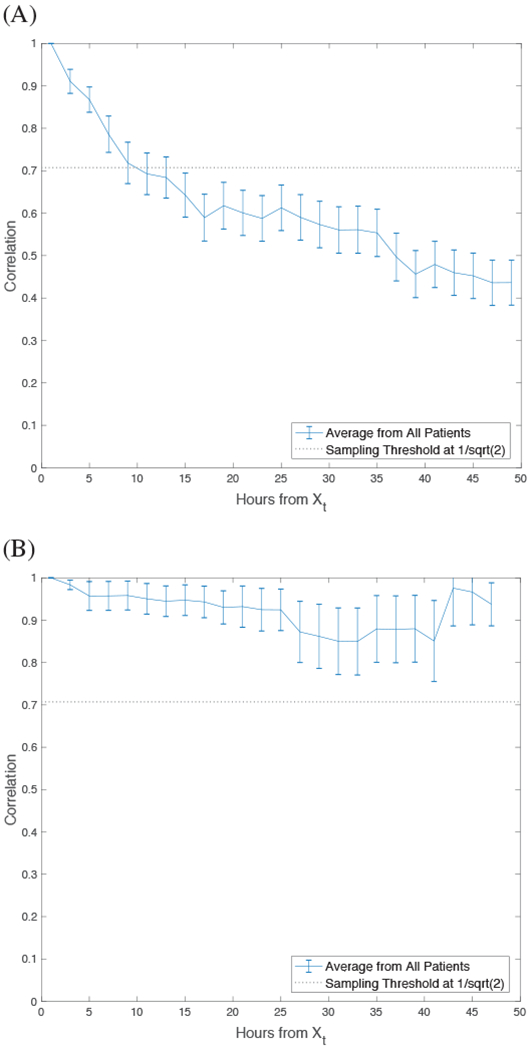
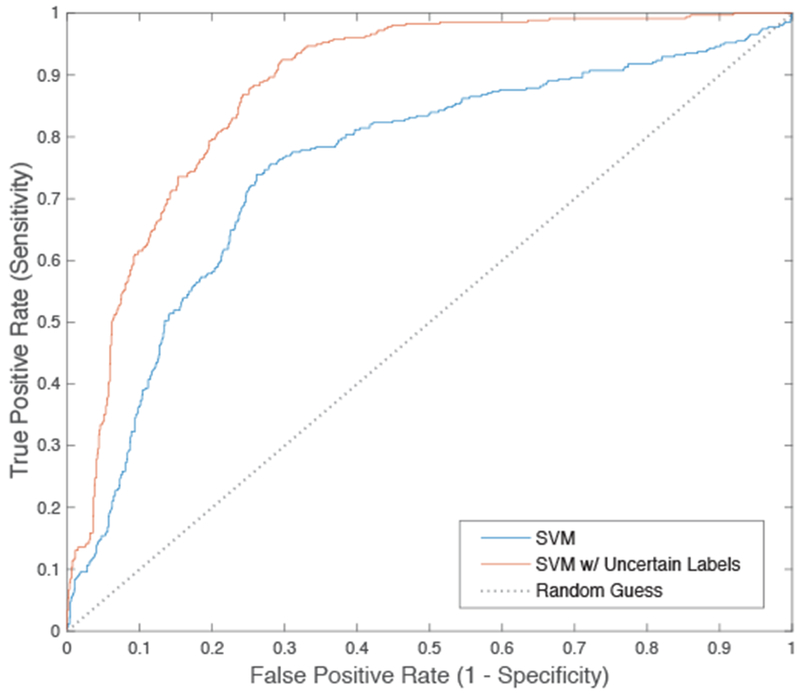
When training a machine learning algorithm for a supervised-learning task in some clinical applications, uncertainty in the correct labels of some patients may adversely affect the performance of the algorithm. For example, even clinical experts may have less confidence when assigning a medical diagnosis to some patients because of ambiguity in the patient's case or imperfect reliability of the diagnostic criteria. As a result, some cases used in algorithm training may be mislabeled, adversely affecting the algorithm's performance. However, experts may also be able to quantify their diagnostic uncertainty in these cases. We present a robust method implemented with support vector machines (SVM) to account for such clinical diagnostic uncertainty when training an algorithm to detect patients who develop the acute respiratory distress syndrome (ARDS). ARDS is a syndrome of the critically ill that is diagnosed using clinical criteria known to be imperfect. We represent uncertainty in the diagnosis of ARDS as a graded weight of confidence associated with each training label. We also performed a novel time-series sampling method to address the problem of intercorrelation among the longitudinal clinical data from each patient used in model training to limit overfitting. Preliminary results show that we can achieve meaningful improvement in the performance of algorithm to detect patients with ARDS on a hold-out sample, when we compare our method that accounts for the uncertainty of training labels with a conventional SVM algorithm.
Figures

References
-
- Rubenfeld GD et al. , Incidence and outcomes of acute lung injury, N Engl J Med, vol. 353(16), pp. 1685–1693. October 2005. - PubMed
-
- Bellani G et al. , Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries, JAMA, vol. 315(8), pp. 788–800. February 2016. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
