

Deep Learning Global Glomerulosclerosis in Transplant Kidney Frozen Sections
- PMID: 29994669
- PMCID: PMC6296264
- DOI: 10.1109/TMI.2018.2851150
Deep Learning Global Glomerulosclerosis in Transplant Kidney Frozen Sections
Abstract
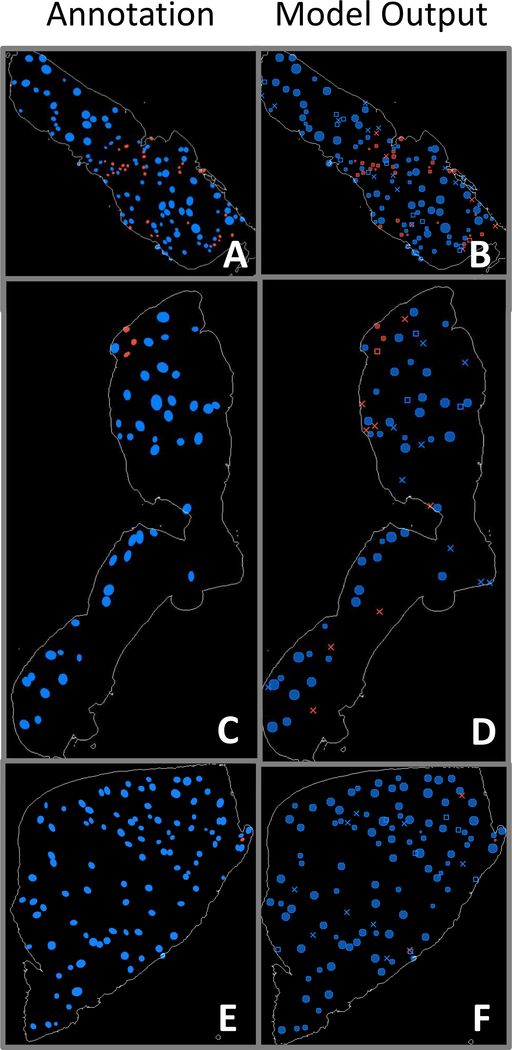
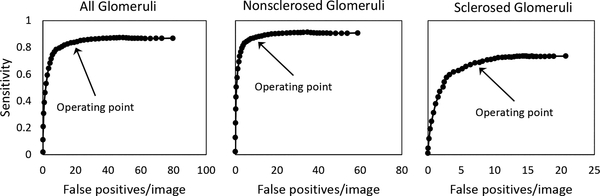
Transplantable kidneys are in very limited supply. Accurate viability assessment prior to transplantation could minimize organ discard. Rapid and accurate evaluation of intra-operative donor kidney biopsies is essential for determining which kidneys are eligible for transplantation. The criterion for accepting or rejecting donor kidneys relies heavily on pathologist determination of the percent of glomeruli (determined from a frozen section) that are normal and sclerotic. This percentage is a critical measurement that correlates with transplant outcome. Inter- and intra-observer variability in donor biopsy evaluation is, however, significant. An automated method for determination of percent global glomerulosclerosis could prove useful in decreasing evaluation variability, increasing throughput, and easing the burden on pathologists. Here, we describe the development of a deep learning model that identifies and classifies non-sclerosed and sclerosed glomeruli in whole-slide images of donor kidney frozen section biopsies. This model extends a convolutional neural network (CNN) pre-trained on a large database of digital images. The extended model, when trained on just 48 whole slide images, exhibits slide-level evaluation performance on par with expert renal pathologists. Encouragingly, the model's performance is robust to slide preparation artifacts associated with frozen section preparation. The model substantially outperforms a model trained on image patches of isolated glomeruli, in terms of both accuracy and speed. The methodology overcomes the technical challenge of applying a pretrained CNN bottleneck model to whole-slide image classification. The traditional patch-based approach, while exhibiting deceptively good performance classifying isolated patches, does not translate successfully to whole-slide image segmentation in this setting. As the first model reported that identifies and classifies normal and sclerotic glomeruli in frozen kidney sections, and thus the first model reported in the literature relevant to kidney transplantation, it may become an essential part of donor kidney biopsy evaluation in the clinical setting.
Figures

References
-
- Jochmans I and Pirenne J, “Graft quality assessment in kidney transplantation: not an exact science yet!” Current Opinion in Organ Transplantation, vol. 16, no. 2, pp. 174–179, April 2011. - PubMed
-
- Remuzzi G, Cravedi P, Perna A, Dimitrov BD, Turturro M, Locatelli G, Rigotti P, Baldan N, Beatini M, Valente U, Scalamogna M, and Ruggenenti P, “Long-term outcome of renal transplantation from older donors.” The New England Journal of Medicine, vol. 354, no. 4, pp. 343–52, January 2006. - PubMed
-
- Munivenkatappa RB, Schweitzer EJ, Papadimitriou JC, Drachenberg CB, Thom KA, Perencevich EN, Haririan A, Rasetto F, Cooper M, Campos L, Barth RN, Bartlett ST, and Philosophe B, “The Maryland Aggregate Pathology Index: A deceased donor kidney biopsy scoring system for predicting graft failure,” American Journal of Transplantation, vol. 8, no. 11, pp. 2316–2324, November 2008. - PubMed
-
- Rege A, Irish B, Castleberry A, Vikraman D, Sanoff S, Ravindra K, Collins B, and Sudan D, “Trends in Usage and Outcomes for Expanded Criteria Donor Kidney Transplantation in the United States Characterized by Kidney Donor Profile Index.” Cureus, vol. 8, no. 11, p. e887, November 2016. - PMC - PubMed
-
- Furness PN and Taub N, “International variation in the interpretation of renal transplant biopsies: Report of the CERTPAP project,” Kidney International, vol. 60, no. 5, pp. 1998–2012, November 2001. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
