

Chest wall effect on the monitoring of respiratory mechanics in acute respiratory distress syndrome
- PMID: 29995087
- PMCID: PMC6031425
- DOI: 10.5935/0103-507X.20180038
Chest wall effect on the monitoring of respiratory mechanics in acute respiratory distress syndrome
Abstract
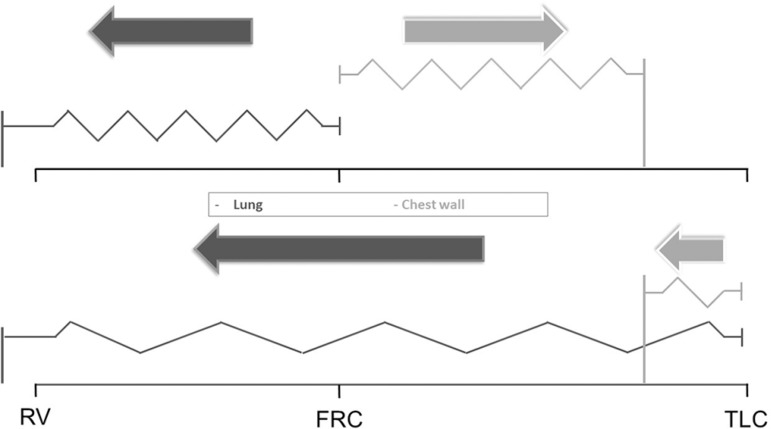
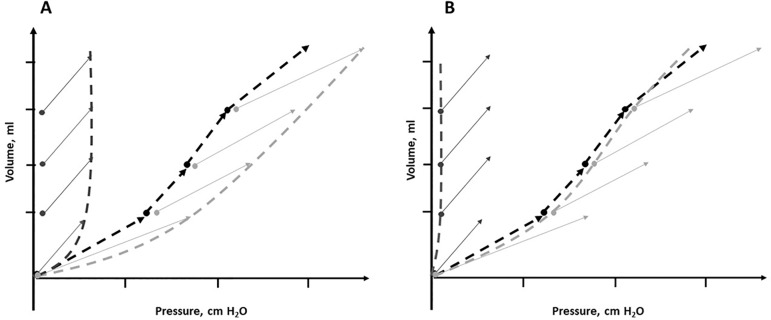
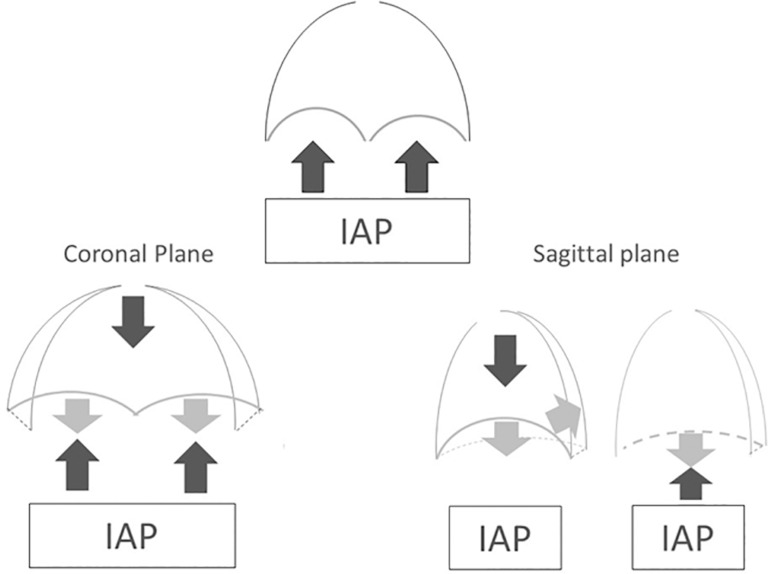
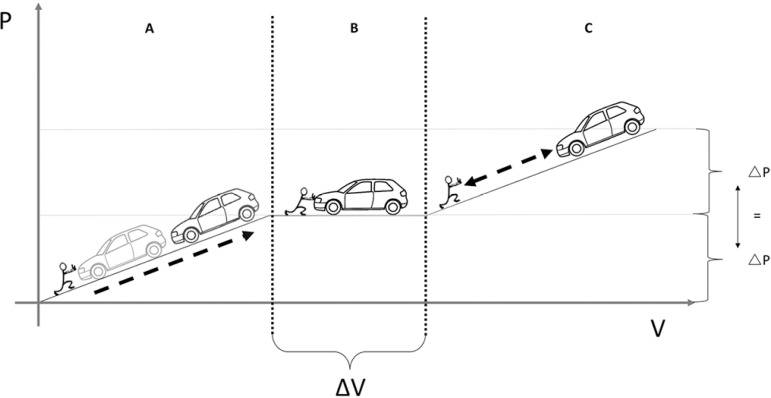
The respiratory system mechanics depend on the characteristics of the lung and chest wall and their interaction. In patients with acute respiratory distress syndrome under mechanical ventilation, the monitoring of airway plateau pressure is fundamental given its prognostic value and its capacity to assess pulmonary stress. However, its validity can be affected by changes in mechanical characteristics of the chest wall, and it provides no data to correctly titrate positive end-expiratory pressure by restoring lung volume. The chest wall effect on respiratory mechanics in acute respiratory distress syndrome has not been completely described, and it has likely been overestimated, which may lead to erroneous decision making. The load imposed by the chest wall is negligible when the respiratory system is insufflated with positive end-expiratory pressure. Under dynamic conditions, moving this structure demands a pressure change whose magnitude is related to its mechanical characteristics, and this load remains constant regardless of the volume from which it is insufflated. Thus, changes in airway pressure reflect changes in the lung mechanical conditions. Advanced monitoring could be reserved for patients with increased intra-abdominal pressure in whom a protective mechanical ventilation strategy cannot be implemented. The estimates of alveolar recruitment based on respiratory system mechanics could reflect differences in chest wall response to insufflation and not actual alveolar recruitment.
La mecánica del sistema respiratorio depende de las características del pulmón, la caja torácica y su interacción. En pacientes con síndrome de distrés respiratorio agudo bajo ventilación mecánica el monitoreo de la presión meseta en la vía aérea es fundamental debido a su valor pronóstico y su capacidad de reflejar el estrés pulmonar. Sin embargo, su validez puede verse afectada por cambios en las características mecánicas de la caja torácica, y además, no otorga información para la correcta titulación de presión positiva al final de la espiración en función de restablecer el volumen pulmonar. La influencia que la caja torácica ejerce sobre la mecánica del sistema respiratorio en síndrome de distrés respiratorio agudo no ha sido completamente descripta y es probable que haya sido sobredimensionada pudiendo conducir a toma de decisiones erróneas. Ante la insuflación con presión positiva al final de la espiración, la carga impuesta por la caja torácica es despreciable. En condiciones dinámicas, desplazar esta estructura demanda un cambio de presión cuya magnitud se relaciona con sus características mecánicas, dicha carga se mantiene constante independientemente del volumen a partir del cual es insuflada. Por lo que cambios en la presión en la vía aérea reflejan modificaciones en las condiciones mecánicas del pulmón. El monitoreo avanzado podría reservarse para pacientes con incremento de la presión intra-abdominal en los que no pueda implementarse una estrategia de ventilación mecánica protectora. Las estimaciones de reclutamiento alveolar basadas en la mecánica del sistema respiratorio podrían ser reflejo del diferente comportamiento de la caja torácica a la insuflación y no verdadero reclutamiento alveolar.
Conflict of interest statement
Figures
Similar articles
-
Lung stress and strain during mechanical ventilation for acute respiratory distress syndrome.Am J Respir Crit Care Med. 2008 Aug 15;178(4):346-55. doi: 10.1164/rccm.200710-1589OC. Epub 2008 May 1. Am J Respir Crit Care Med. 2008. PMID: 18451319
-
The chest wall in acute lung injury/acute respiratory distress syndrome.Curr Opin Crit Care. 2008 Feb;14(1):94-102. doi: 10.1097/MCC.0b013e3282f40952. Curr Opin Crit Care. 2008. PMID: 18195633 Review.
-
Monitoring of pulmonary mechanics in acute respiratory distress syndrome to titrate therapy.Curr Opin Crit Care. 2005 Jun;11(3):252-8. doi: 10.1097/01.ccx.0000160773.43122.35. Curr Opin Crit Care. 2005. PMID: 15928475 Review.
-
Recruitment maneuvers and positive end-expiratory pressure/tidal ventilation titration in acute lung injury/acute respiratory distress syndrome: translating experimental results to clinical practice.Crit Care. 2005 Oct 5;9(5):424-6. doi: 10.1186/cc3800. Epub 2005 Aug 18. Crit Care. 2005. PMID: 16277726 Free PMC article.
-
Airway driving pressure and lung stress in ARDS patients.Crit Care. 2016 Aug 22;20:276. doi: 10.1186/s13054-016-1446-7. Crit Care. 2016. PMID: 27545828 Free PMC article.
Cited by
-
Airway and Transpulmonary Driving Pressure by End-Inspiratory Holds During Pressure Support Ventilation.Respir Care. 2023 Nov;68(11):1483-1492. doi: 10.4187/respcare.10802. Epub 2023 Jul 18. Respir Care. 2023. PMID: 37463722 Free PMC article.
-
Thoracic cavity remodeling and pulmonary function change after chest wall resection.J Thorac Dis. 2024 May 31;16(5):2723-2735. doi: 10.21037/jtd-24-25. Epub 2024 May 8. J Thorac Dis. 2024. PMID: 38883658 Free PMC article.
References
-
- Acute Respiratory Distress Syndrome Network. Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–1308. - PubMed
-
- Estenssoro E, Ríos FG, Apezteguía C, Reina R, Neira J, Ceraso DH, Orlandi C, Valentini R, Tiribelli N, Brizuela M, Balasini C, Mare S, Domeniconi G, Ilutovich S, Gómez A, Giuliani J, Barrios C, Valdez P, Registry of the Argentinian Society of Intensive Care SATI Pandemic 2009 influenza A in Argentina: a study of 337 patients on mechanical ventilation. Am J Respir Crit Care Med. 2010;182(1):41–48. - PubMed
-
- Henderson WR, Chen L, Amato MB, Brochard LJ. Fifty years of research in ARDS. Respiratory mechanics in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;196(7):822–833. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
