

Comparison of the predictive value of scoring systems on the prognosis of cirrhotic patients with suspected infection
- PMID: 29995791
- PMCID: PMC6076170
- DOI: 10.1097/MD.0000000000011421
Comparison of the predictive value of scoring systems on the prognosis of cirrhotic patients with suspected infection
Abstract
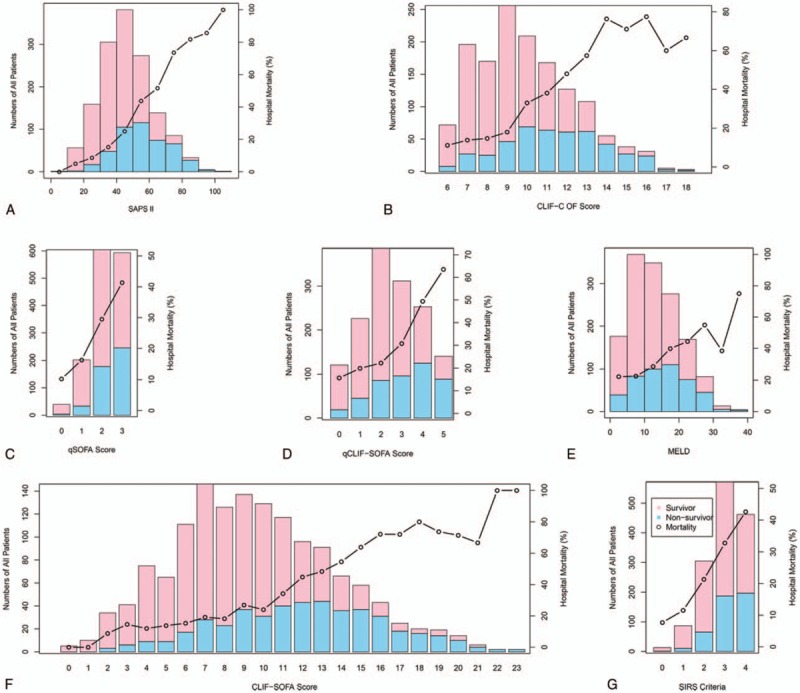
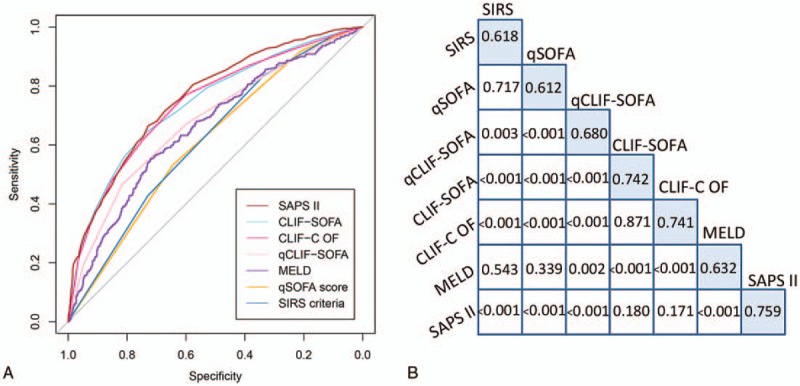
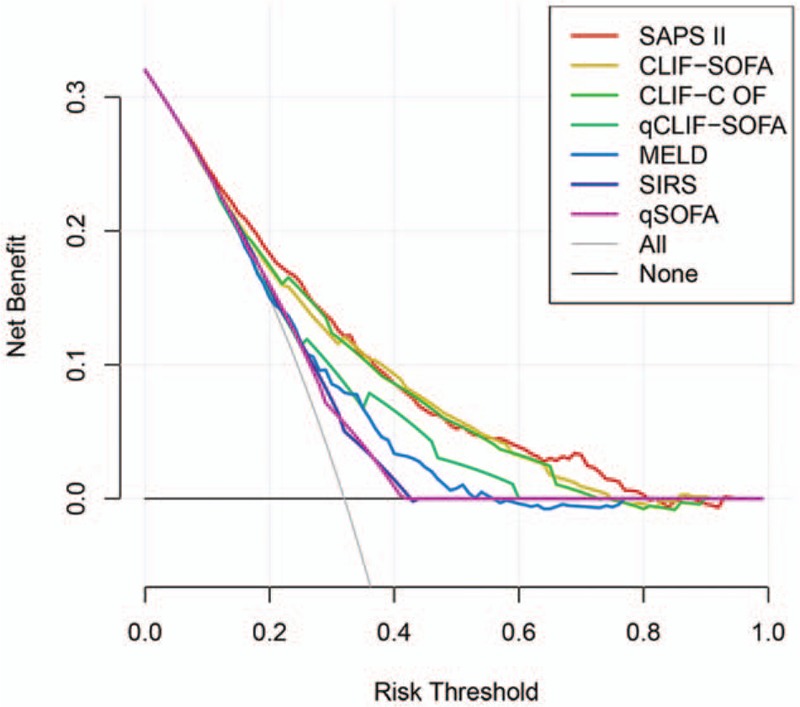
Cirrhotic patients with infection are prone to develop sepsis or even septic shock rendering poorer prognosis. However, few methods are available to predict the prognosis of cirrhotic patients with infection although there are some scoring systems can be used to predict general patients with cirrhosis. Therefore, we aimed to explore the predictive value of scoring systems in determining the outcome of critically ill cirrhotic patients with suspected infection.This was a retrospective cohort study based on a single-center database. The prognostic accuracy of the systemic inflammatory response syndrome (SIRS) criteria, quick Sequential Organ Failure Assessment (qSOFA), chronic liver failure (CLIF)-SOFA, quick CLIF-SOFA (qCLIF-SOFA), CLIF-consortium organ failure (CLIF-C OF), Model for End-Stage Liver Disease (MELD), and Simplified Acute Physiology Score (SAPS) II were compared by using area under the receiver operating characteristic (AUROC) curve and net benefit with decision curve analysis. The primary endpoint was in-hospital mortality while the secondary endpoints were duration of hospital and intensive care unit (ICU) stay and ICU mortality.A total of 1438 cirrhotic patients with suspected infection were included in the study. Nearly half the patients (50.2%) were admitted to the ICU due to hepatic encephalopathy and the overall in-hospital mortality was 32.0%. Hospital and ICU mortality increased as the score of each scoring system increased (P < .05 for all trends). The AUROC of CLIF-SOFA (AUROC, 0.742; 95% confidence interval, CI, 0.714-0.770), CLIF-C OF (AUROC, 0.741; 95% CI, 0.713-0.769), and SAPS II (AUROC, 0.759; 95% CI, 0.733-0.786) were significantly higher than SIRS criteria (AUROC, 0.618; 95% CI, 0.590-0.647), qSOFA (AUROC, 0.612; 95% CI, 0.584-0.640), MELD (AUROC, 0.632; 95% CI, 0.601-0.662), or qCLIF-SOFA (AUROC, 0.680; 95% CI, 0.650-0.710) (P < .05 for all). In the decision curve analysis, the net benefit of implementing CLIF-SOFA and CLIF-C OF to predict the prognosis of cirrhotic patients with suspected infection were higher compared with SIRS, qSOFA, MELD, or qCLIF-SOFA.CLIF-SOFA and CLIF-C OF scores, as well as SAPS II were better tools than SIRS, qSOFA, MELD, or qCLIF-SOFA to evaluate the prognosis of critically ill cirrhotic patients with suspected infection.
Conflict of interest statement
The authors declare no conflicts of interests.
Figures
Similar articles
-
Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults With Suspected Infection Admitted to the Intensive Care Unit.JAMA. 2017 Jan 17;317(3):290-300. doi: 10.1001/jama.2016.20328. JAMA. 2017. PMID: 28114553
-
Quick chronic liver failure-sequential organ failure assessment: an easy-to-use scoring model for predicting mortality risk in critically ill cirrhosis patients.Eur J Gastroenterol Hepatol. 2017 Jun;29(6):698-705. doi: 10.1097/MEG.0000000000000856. Eur J Gastroenterol Hepatol. 2017. PMID: 28240612
-
Establishment of MELD-lactate clearance scoring system in predicting death risk of critically ill cirrhotic patients.BMC Gastroenterol. 2022 Jun 3;22(1):280. doi: 10.1186/s12876-022-02351-5. BMC Gastroenterol. 2022. PMID: 35658837 Free PMC article.
-
Advances in management and prognostication in critically ill cirrhotic patients.Curr Opin Crit Care. 2014 Apr;20(2):210-7. doi: 10.1097/MCC.0000000000000067. Curr Opin Crit Care. 2014. PMID: 24514101 Review.
-
Accuracy of quick Sequential Organ Failure Assessment (qSOFA) score and systemic inflammatory response syndrome (SIRS) criteria for predicting mortality in hospitalized patients with suspected infection: a meta-analysis of observational studies.Clin Microbiol Infect. 2018 Nov;24(11):1123-1129. doi: 10.1016/j.cmi.2018.03.032. Epub 2018 Mar 29. Clin Microbiol Infect. 2018. PMID: 29605565
Cited by
-
Management of sepsis in a cirrhotic patient admitted to the intensive care unit: A systematic literature review.World J Hepatol. 2023 Jun 27;15(6):850-866. doi: 10.4254/wjh.v15.i6.850. World J Hepatol. 2023. PMID: 37397933 Free PMC article.
-
Relationship Between Etiology of Cirrhosis and Survival Among Patients Hospitalized in Intensive Care Units.Mayo Clin Proc. 2022 Feb;97(2):274-284. doi: 10.1016/j.mayocp.2021.08.025. Epub 2022 Jan 25. Mayo Clin Proc. 2022. PMID: 35090753 Free PMC article.
-
Prognostic value of von-Willebrand factor in patients with liver cirrhosis and its relation to other prognostic indicators.World J Hepatol. 2022 Apr 27;14(4):812-826. doi: 10.4254/wjh.v14.i4.812. World J Hepatol. 2022. PMID: 35646274 Free PMC article.
-
Cirrhotic Patients on Mechanical Ventilation Have a Low Rate of Successful Extubation and Survival.Dig Dis Sci. 2020 Dec;65(12):3744-3752. doi: 10.1007/s10620-020-06051-6. Epub 2020 Jan 20. Dig Dis Sci. 2020. PMID: 31960201 Free PMC article.
-
Development of a quantitative index system for evaluating the quality of electronic medical records in disease risk intelligent prediction.BMC Med Inform Decis Mak. 2024 Jun 24;24(1):178. doi: 10.1186/s12911-024-02533-z. BMC Med Inform Decis Mak. 2024. PMID: 38915008 Free PMC article.
References
-
- Gustot T, Fernandez J, Szabo G, et al. Sepsis in alcohol-related liver disease. J Hepatol 2017;67:1031–50. - PubMed
-
- Fernandez J, Acevedo J, Castro M, et al. Prevalence and risk factors of infections by multiresistant bacteria in cirrhosis: a prospective study. Hepatology 2012;55:1551–61. - PubMed
-
- Winters BD, Eberlein M, Leung J, et al. Long-term mortality and quality of life in sepsis: a systematic review. Crit Care Med 2010;38:1276–83. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
