

Pachychoroid disease
- PMID: 29995841
- PMCID: PMC6328576
- DOI: 10.1038/s41433-018-0158-4
Pachychoroid disease
Abstract
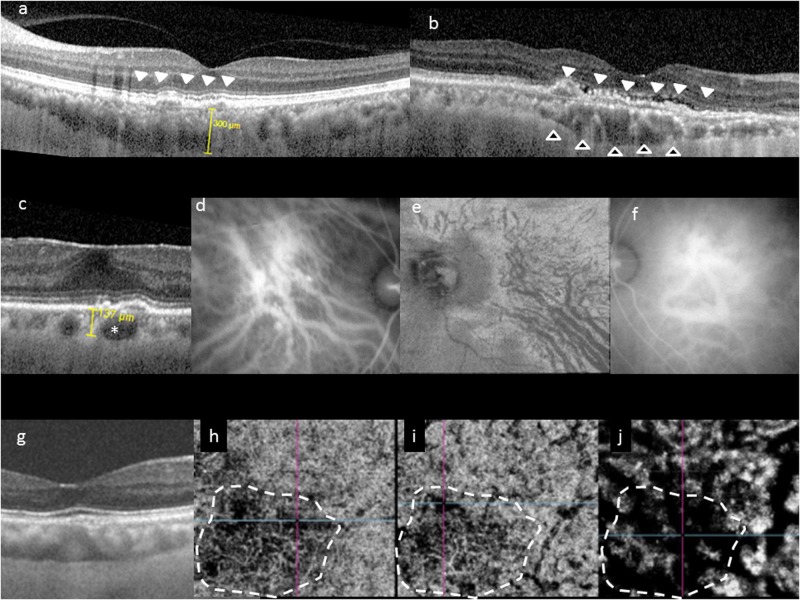
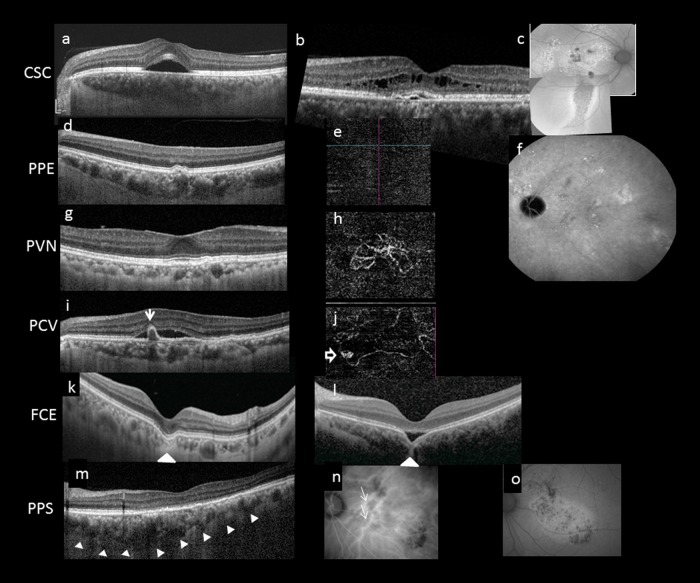
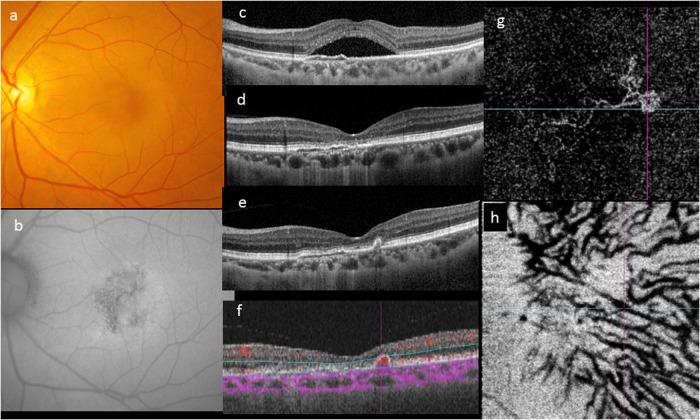
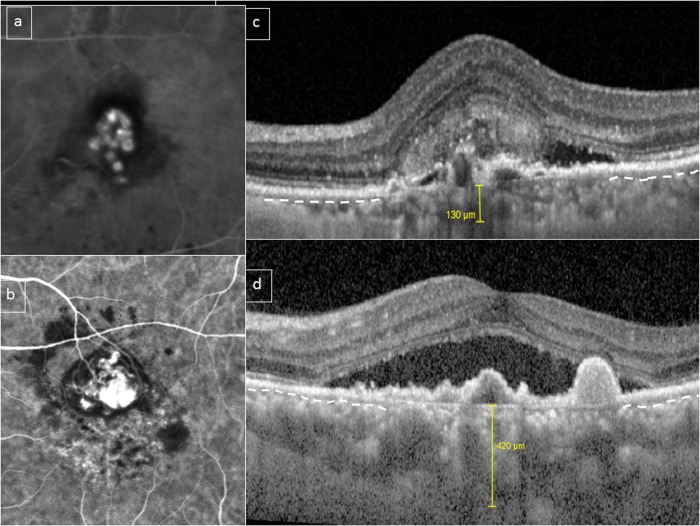
Pachychoroid is a relatively novel concept describing a phenotype characterized by attenuation of the choriocapillaris overlying dilated choroidal veins, and associated with progressive retinal pigment epithelium dysfunction and neovascularization. The emphasis in defining pachychoroid-related disorders has shifted away from simply an abnormally thick choroid (pachychoroid) toward a detailed morphological definition of a pathologic state (pachychoroid disease) with functional implications, which will be discussed in this review. Several clinical manifestations have been described to reside within the pachychoroid disease spectrum, including central serous chorioretinopathy, pachychoroid pigment epitheliopathy, pachychoroid neovasculopathy, polypoidal choroidal vasculopathy/aneurysmal type 1 neovascularization, focal choroidal excavation, peripapillary pachychoroid syndrome. These conditions all exhibit the characteristic choroidal alterations and are believed to represent different manifestations of a common pathogenic process. This review is based on both the current literature and the clinical experience of our individual authors, with an emphasis on the clinical and imaging features, management considerations, as well as current understanding of pathogenesis of these disorders within the context of the recent findings related to pachychoroid disease.
摘要: 肥厚型脉络膜疾病是近年来提出的新概念, 其描述了一类特征为脉络膜毛细血管层的静脉扩张, 并且与进行性视网膜色素上皮功能障碍和新生血管的形成有关的一类疾病。定义肥厚型脉络膜相关疾病的重点已经从简单的脉络膜厚度异常 (脉络膜肥厚) 转向影响功能的病理状态 (“肥厚型脉络膜疾病”) 的详细形态学定义, 这将在本综述中详细讨论。属于肥厚型脉络膜疾病谱的疾病, 包括中心性浆液性脉络膜视网膜病变, 肥厚型脉络膜色素上皮病变, 肥厚型脉络膜新生血管病变, 息肉状脉络膜血管病变/1型动脉瘤新生血管, 局灶性脉络膜凹陷, 视盘周围毛细脉络膜肥厚综合症。这些病症都表现出特征性的脉络膜改变, 并且被认为代表了常见致病过程的不同临床表现。 本综述基于目前已发表的文献和作者自身的临床经验以及最近在肥厚型脉络疾病的相关研究结果, 重点强调了临床表现、影像学特征、治疗要点以及目前对这些疾病发病机制的探讨。.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Mrejen S, Spaide RF. Optical coherence tomography: imaging of the choroid and beyond. Surv Ophthalmol. 2013;58:387–429. - PubMed
-
- Yanagi Y, Ting DSW, Ng WY, et al. Choroidal vascular hyperpermeability as a predictor of treatment response for polypoidal choroidal vasculopathy. Retina. 2017 Jul 12. Epub ahead of print. - PubMed
-
- Guyer DR, Yannuzzi LA, Slakter JS, Sorenson JA, Hope-Ross M, Orlock DR. Digital indocyanine-green videoangiography of occult choroidal neovascularization. Ophthalmology. 1994;101:1727–35. - PubMed
-
- Dansingani KK, Balaratnasingam C, Naysan J, Freund KB. En face imaging of pachychoroid spectrum disorders with swept-source optical coherence tomography. Retina. 2016;36:499–516. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
