

Prevention of laparoscopic surgery induced hypothermia with warmed humidified insufflation: Is the experimental combination of a warming blanket synergistic?
- PMID: 29995891
- PMCID: PMC6040690
- DOI: 10.1371/journal.pone.0199369
Prevention of laparoscopic surgery induced hypothermia with warmed humidified insufflation: Is the experimental combination of a warming blanket synergistic?
Abstract
Introduction: Maintaining normothermia during anesthesia is imperative to provide quality patient care and to prevent adverse outcomes. Prolonged laparoscopic procedures have been identified as a potential risk factor for hypothermia, due to continuous insufflation of cold and dry carbon dioxide. Perioperative hypothermia is associated with increased hospital cost and many complications including; impaired drug metabolism, impaired immune function, cardiac morbidity, shivering, coagulopathy.
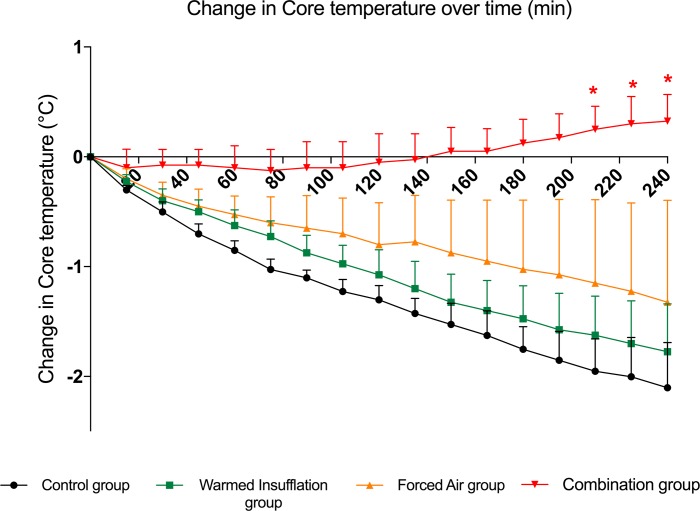
Methods: In this experimental study, four pigs underwent four interventions each, resulting in 16 total trials. Using standardized general anesthesia in a randomized Latin-square sequence the four interventions include: 1. Control group without an administered pneumoperitoneum, 2. Administered standard pneumoperitoneum using 21°C insufflated gas and under-body forced-air warming, 3. Administered pneumoperitoneum with insufflation of warmed/humidified carbon dioxide, 4. Administered pneumoperitoneum with insufflation of warmed/humidified carbon dioxide and under-body forced-air warming. The primary outcome was distal esophageal temperature change 4 hours after trocar insertion.
Results: Four hours after trocar insertion, pigs in the control group lost 2.1 ± 0.4°C; pigs with warmed and humidified insufflation lost 1.8 ± 0.4°C; pigs with forced-air warming group lost 1.3 ± 0.9°C; and pigs exposed to a combination of warmed and humidified insufflation with forced-air warming increased by 0.3 ± 0.2°C.
Conclusion: This experimental animal study provides evidence that a combination of warmed and humidified insufflation of carbon dioxide (CO2) in conjunction with forced-air warming is an effective strategy in the prevention of perioperative hypothermia. Further clinical trials investigating humans are therefore indicated.
Conflict of interest statement
Laparoscopic Humigard insufflators were provided for free by Fisher & Paykel HealthCare. Pierre Diemunsch reported his participation in a research meeting sponsored by Fisher & Paykel in 2013. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Cheng C, Matsukawa T, Sessler DI, Ozaki M, Kurz A, Merrifield B, et al. Increasing mean skin temperature linearly reduces the core-temperature thresholds for vasoconstriction and shivering in humans. Anesthesiology. 1995;82(5):1160–8. Epub 1995/05/01. . - PubMed
-
- Frank SM, Fleisher LA, Breslow MJ, Higgins MS, Olson KF, Kelly S, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA. 1997;277(14):1127–34. Epub 1997/04/09. . - PubMed
-
- Lenhardt R, Marker E, Goll V, Tschernich H, Kurz A, Sessler DI, et al. Mild intraoperative hypothermia prolongs postanesthetic recovery. Anesthesiology. 1997;87(6):1318–23. Epub 1998/01/07. . - PubMed
-
- Michelson AD, MacGregor H, Barnard MR, Kestin AS, Rohrer MJ, Valeri CR. Reversible inhibition of human platelet activation by hypothermia in vivo and in vitro. Thromb Haemost. 1994;71(5):633–40. Epub 1994/05/01. . - PubMed
-
- Wenisch C, Narzt E, Sessler DI, Parschalk B, Lenhardt R, Kurz A, et al. Mild intraoperative hypothermia reduces production of reactive oxygen intermediates by polymorphonuclear leukocytes. Anesth Analg. 1996;82(4):810–6. Epub 1996/04/01. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
