

Self-reported health behaviors, including sleep, correlate with doctor-informed medical conditions: data from the 2011 Health Related Behaviors Survey of U.S. Active Duty Military Personnel
- PMID: 29996814
- PMCID: PMC6042384
- DOI: 10.1186/s12889-018-5781-2
Self-reported health behaviors, including sleep, correlate with doctor-informed medical conditions: data from the 2011 Health Related Behaviors Survey of U.S. Active Duty Military Personnel
Abstract
Background: Health behaviors and cardiometabolic disease risk factors may differ between military and civilian populations; therefore, in U.S. active duty military personnel, we assessed relationships between demographic characteristics, self-reported health behaviors, and doctor-informed medical conditions.
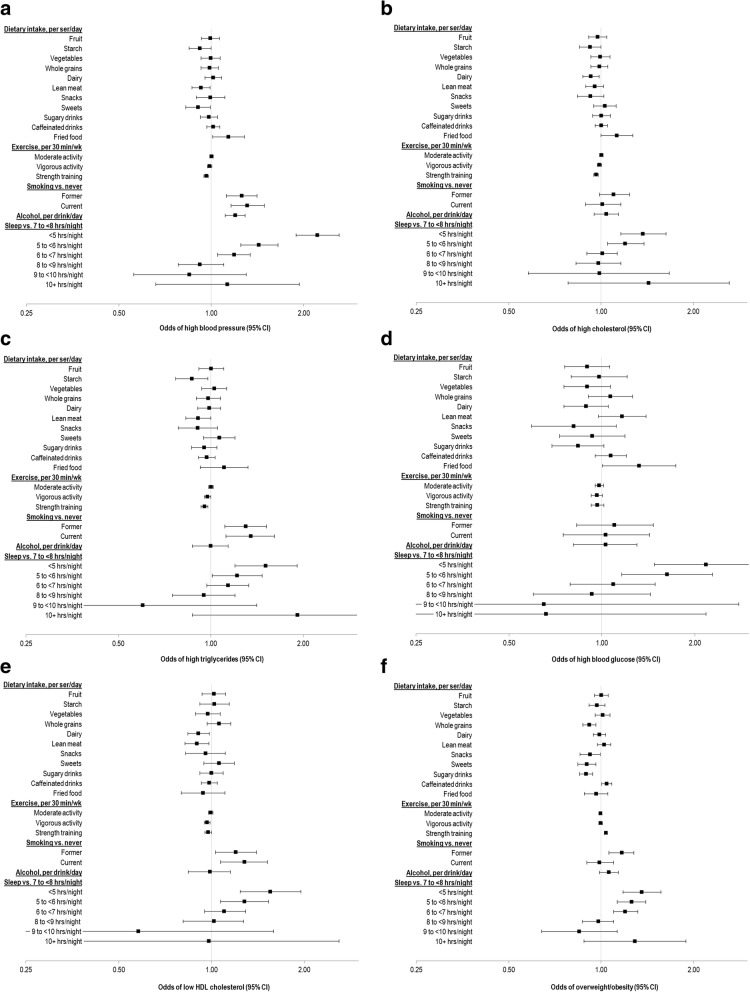
Methods: Data were self-reported by 27,034 active duty military and Coast Guard personnel who responded to the 2011 Department of Defense Health Related Behaviors Survey. Multivariate linear and logistic regressions were used to estimate cross-sectional associations between (1) demographic characteristics (age, sex, service branch, marital status, children, race/ethnicity, pay grade) and self-reported behaviors (exercise, diet, smoking, alcohol, sleep); (2) demographic characteristics and doctor-informed medical conditions (hypertension, hypercholesterolemia, low high density lipoprotein (HDL) cholesterol, hyperglycemia) and overweight/obesity; and (3) behaviors and doctor-informed medical conditions.
Results: Among respondents (age 29.9 ± 0.1 years, 14.7% female), females reported higher intake than men of fruit, vegetables, and dairy; those with higher education reported higher intakes of whole grains; those currently married and/or residing with children reported higher intake of starches. Older age and female sex were associated with higher odds (ORs 1.25 to 12.54 versus the youngest age group) of overweight/obesity. Older age and female sex were also associated with lower odds (ORs 0.29 to 0.65 versus male sex) of doctor-informed medical conditions, except for blood glucose, for which females had higher odds. Those currently married had higher odds of high cholesterol and overweight/obesity, and separated/divorced/widowed respondents had higher odds of high blood pressure and high cholesterol. Short sleep duration (< 5 versus 7-8 h/night) was associated with higher odds (ORs 1.36to 2.22) of any given doctor-informed medical condition. Strength training was associated with lower probability of high cholesterol, high triglycerides, and low HDL, and higher probability of overweight/obesity. Dietary factors were variably associated with doctor-informed medical conditions and overweight/obesity.
Conclusions: This study observed pronounced associations between health behaviors-especially sleep-and medical conditions, thus adding to evidence that sleep is a critical, potentially modifiable behavior within this population. When possible, adequate sleep should continue to be promoted as an important part of overall health and wellness throughout the military community.
Keywords: Air force; Army; Cardiometabolic risk; Coast guard; Exercise; Marine corps; Navy; Sleep; Survey.
Conflict of interest statement
Ethics approval and consent to participate
The 2011 HRBS was conducted by ICF International under advisement of the Office of the Assistant Secretary of Defense for Health Affairs, Tricare Management Activity (TMA; now Defense Health Agency), and the USCG [15]. Primary data collection was approved by the Office of the Assistant Secretary of Defense for Health Affairs/TRICARE Management Activity (OASD(HA)/TMA), Human Research Protection Office. Informed consent was required and obtained at the beginning of the HRBS, and responses were anonymous. For the present secondary data analyses, we obtained a de-identified data file from TMA through a data use agreement. Because the data were previously collected and de-identified, the protocol for the present study was deemed exempt (not human subject research) by both the US Army Research Institute of Environmental Medicine (Natick, MA) and the Office of the Assistant Secretary of Defense for Health Affairs/TRICARE Management Activity (OASD(HA)/TMA), Human Research Protection Office.
Consent for publication
Not applicable (no individual-level data included).
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Behavioral correlates of self-reported health status in US active duty military.Prev Med. 2020 Feb;131:105930. doi: 10.1016/j.ypmed.2019.105930. Epub 2019 Nov 22. Prev Med. 2020. PMID: 31765709
-
Predictors of Wellness Behaviors in U.S. Army Physicians.Mil Med. 2018 Nov 1;183(11-12):e641-e648. doi: 10.1093/milmed/usy059. Mil Med. 2018. PMID: 29912440
-
Health and health behavior differences: U.S. Military, veteran, and civilian men.Am J Prev Med. 2012 Nov;43(5):483-9. doi: 10.1016/j.amepre.2012.07.029. Am J Prev Med. 2012. PMID: 23079170
-
Sleep Health in U.S. Military Women: A Scoping Review of the Literature, 2000-2019.Womens Health Issues. 2021 Aug 25;31 Suppl 1:S22-S32. doi: 10.1016/j.whi.2021.03.001. Womens Health Issues. 2021. PMID: 34454701
-
Selected weight management interventions for military populations in the United States: a narrative report.Nutr Health. 2017 Jun;23(2):67-74. doi: 10.1177/0260106017704797. Epub 2017 Apr 21. Nutr Health. 2017. PMID: 28429642 Review.
Cited by
-
Sleep disturbances and psychological well-being among military medical doctors of the Swiss Armed Forces: study protocol, rationale and development of a cross-sectional and longitudinal interventional study.Front Public Health. 2024 Aug 6;12:1390636. doi: 10.3389/fpubh.2024.1390636. eCollection 2024. Front Public Health. 2024. PMID: 39171319 Free PMC article.
-
Sleep Duration and Blood Pressure: Recent Advances and Future Directions.Curr Hypertens Rep. 2019 Apr 5;21(5):33. doi: 10.1007/s11906-019-0938-7. Curr Hypertens Rep. 2019. PMID: 30953237 Free PMC article. Review.
-
The Promise of Digital Health: Then, Now, and the Future.NAM Perspect. 2022 Jun 27;2022:10.31478/202206e. doi: 10.31478/202206e. eCollection 2022. NAM Perspect. 2022. PMID: 36177208 Free PMC article. Review. No abstract available.
-
Exercise Dose Associated With Military Service: Implications for the Clinical Management of Inherited Risk for Arrhythmogenic Right Ventricular Cardiomyopathy.Mil Med. 2020 Sep 18;185(9-10):e1447-e1452. doi: 10.1093/milmed/usaa185. Mil Med. 2020. PMID: 32666089 Free PMC article.
-
Impact of Sleep Profiles on Multimorbidity Among US Active-Duty Service Members in the 2018 Health-Related Behaviors Survey.Nat Sci Sleep. 2023 Dec 5;15:1019-1032. doi: 10.2147/NSS.S434813. eCollection 2023. Nat Sci Sleep. 2023. PMID: 38075393 Free PMC article.
References
-
- Survey of Health Related Behaviors [Internet]. Military Health System. [cited 2016 Nov 16]. Available from: https://health.mil/Military-Health-Topics/Access-Cost-Quality-and-Safety....
-
- Smith TJ, Dotson LE, Young AJ, White A, Hadden L, Bathalon GP, Funderburk L, Marriott BP. Eating patterns and leisure-time exercise among active duty military personnel: comparison to the healthy people objectives. J Acad Nutr Diet. 2013;113(7):907–919. doi: 10.1016/j.jand.2013.03.002. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
