

Single cut distal femoral osteotomy for correction of femoral torsion and valgus malformity in patellofemoral malalignment - proof of application of new trigonometrical calculations and 3D-printed cutting guides
- PMID: 29996839
- PMCID: PMC6042371
- DOI: 10.1186/s12891-018-2140-5
Single cut distal femoral osteotomy for correction of femoral torsion and valgus malformity in patellofemoral malalignment - proof of application of new trigonometrical calculations and 3D-printed cutting guides
Abstract
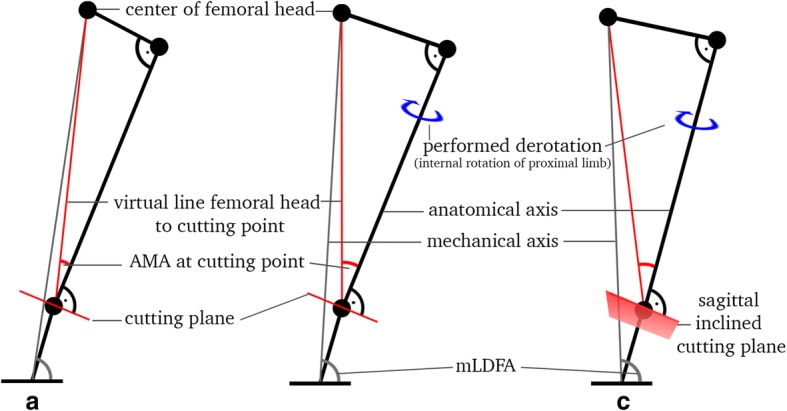
Background: The purpose of this study was to perform a derotational osteotomy at the distal femur, as is done in cases of patellofemoral instability, and demonstrate the predictability of three-dimensional (3D) changes on axes in a cadaveric model by the use of a new mathematical approach.
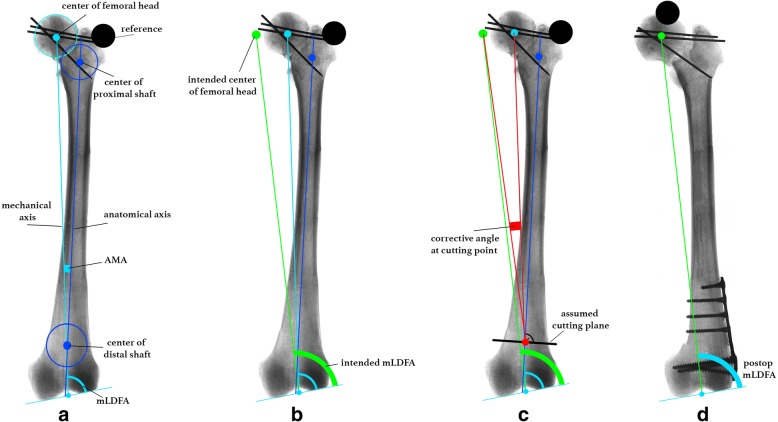
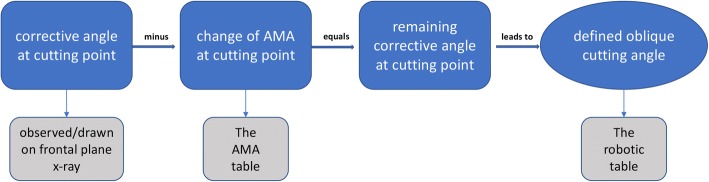
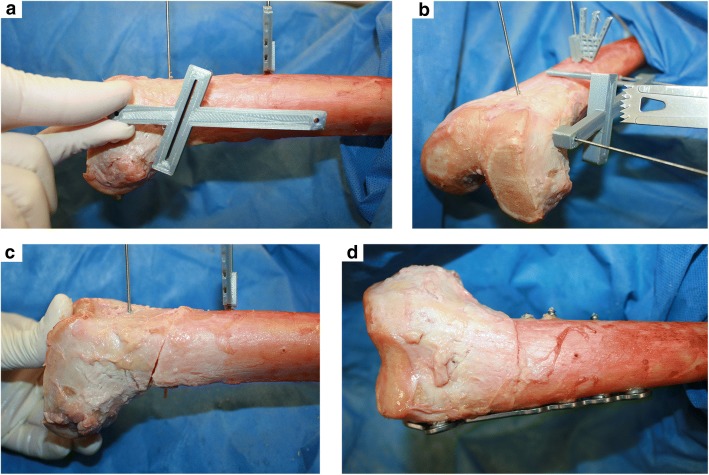
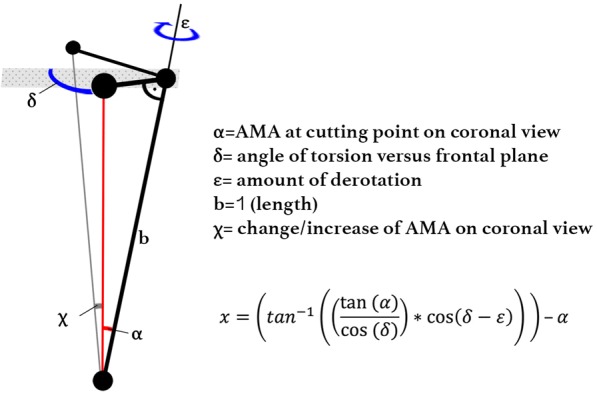
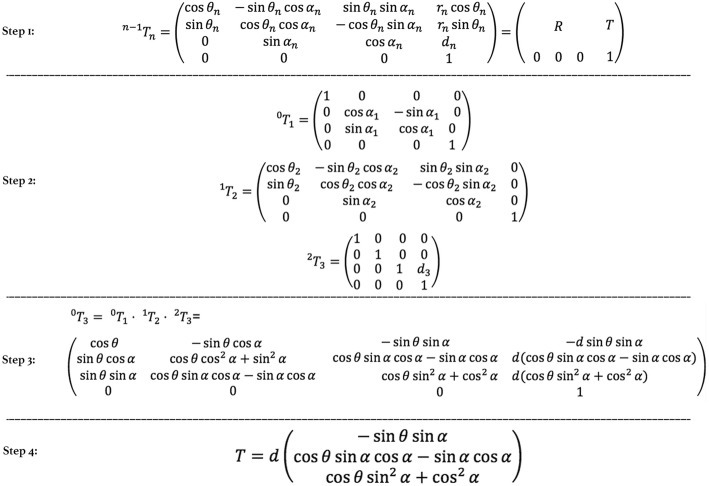
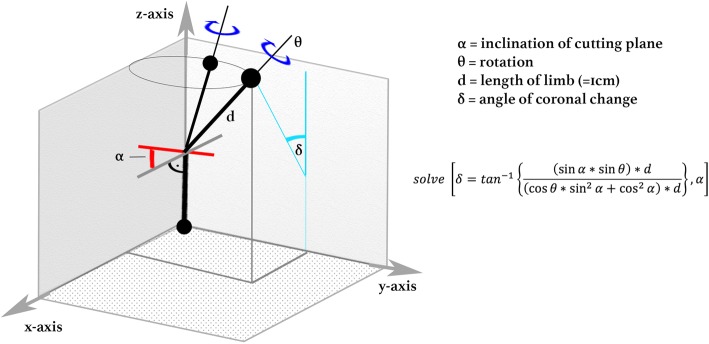
Methods: Ten human cadaveric femurs, with increased antetorsion, underwent a visually observed derotational osteotomy at the distal femur by 20°, as is commonly done in clinics. For surgery, a single cut osteotomy with a defined cutting angle was calculated and given using a simple 3D-printed cutting guide per specimen, based on a newly-created trigonometrical model. To simulate post-operative straight frontal alignment in a normal range, a goal for the mechanical lateral distal femur angle (mLDFA) was set to 87.0° for five specimens (87-goal group) and 90.0° for five specimens (90-goal group). Specimens underwent pre- and post-operative radiographic analysis with CT scan for torsion and frontal plane x-ray for alignment measurements of mLDFA and anatomical mechanical angle (AMA).
Results: Performed derotation showed a mean of 19.69° ±1.08°SD (95% CI: 18.91° to 20.47°). Regarding frontal alignment, a mean mLDFA of 86.9° ±0.66°SD (87-goal-group) and 90.42° ±0.25° SD (90-goal group), was observed (p = 0.008). Overall, the mean difference between intended mLDFA-goal and post-operatively achieved mLDFA was 0.14° ±0.56° SD (95% CI: -0.26° to 0.54°).
Conclusion: A preoperative calculated angle for single cut derotational osteotomy at the distal femur leads to a clinically precise post-operative result on torsion and frontal alignment when using this approach.
Conflict of interest statement
Authors’ information
Florian B. Imhoff, MD; Specialist Orthopaedic and Trauma Surgery; German Board Certified Currently: Postdoctoral Research Fellow at Uconn Health, Department of Orthopaedic Surgery 263 Farmington Avenue, Farmington, CT 06030, USA.
Ethics approval and consent to participate
The study was reported to the institutional review board (IRB) of the Uconn Health, University of Connecticut, and it was documented that no IRB approval was required (de-identified specimen do not constitute human subjects research). Specimen had been obtained from MedCure (MedCure, Inc., Cumberland, RI, USA). According to the distributors information, consent was obtained from the patient before death.
Consent for publication
Not applicable.
Competing interests
Authors IFB, SJ, MA, DT, SB declare that they have no conflict of interest and nothing to disclose.
Author BS is a consultant for Arthrex.
Author IAB is a consultant for Arthrosurface, Arthrex, and mediBayreuth.
Author ARA received an educational and institutional grant from Arthrex and is a consultant for Biorez.
Author BK is a consultant for Arthrex.
No-one of the above-mentioned authors has received personal financial support related to this study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Nelitz M, Dreyhaupt J, Williams SR, Dornacher D. Combined supracondylar femoral derotation osteotomy and patellofemoral ligament reconstruction for recurrent patellar dislocation and severe femoral anteversion syndrome: surgical technique and clinical outcome. Int Orthop. 2015;39:2355–2362. doi: 10.1007/s00264-015-2859-7. - DOI - PubMed
-
- Eckhoff DG, Montgomery WK, Kilcoyne RF, Stamm ER. Femoral morphometry and anterior knee pain. Clin Orthop Relat Res. 1994;(302):64–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
