

Salvage pembrolizumab added to kinase inhibitor therapy for the treatment of anaplastic thyroid carcinoma
- PMID: 29996921
- PMCID: PMC6042271
- DOI: 10.1186/s40425-018-0378-y
Salvage pembrolizumab added to kinase inhibitor therapy for the treatment of anaplastic thyroid carcinoma
Abstract
Background: Anaplastic thyroid carcinoma (ATC) is a rare but deadly form of thyroid cancer. Kinase inhibitors kinase inhibitors have shown clinical efficacy in the management of ATC, however, eventually these tumors acquire resistance to KI and patients succumb to their disease. Salvage therapy in this setting is limited. As ATC tumors diffusely express the programmed cell death protein ligand (PD-L1), anti- programmed cell death protein (PD-1) drugs such as pembrolizumab offer therapeutic potential. We sought to explore the efficacy of adding pembrolizumab to kinase inhibitors at progression in ATC.
Methods: We retrospectively reviewed the charts of ATC patients initiated on pembrolizumab in combination with KI at the time of progression on kinase inhibitors at MD Anderson Cancer Center between August 2016 and August 2017. Efficacy was evaluated with best overall response (BOR) using RECISTv1.1 criteria. Progression free survival (PFS) from the start of pembrolizumab and overall survival (OS) from the start of kinase inhibitors, as well as from the time of addition of pembrolizumab were calculated.
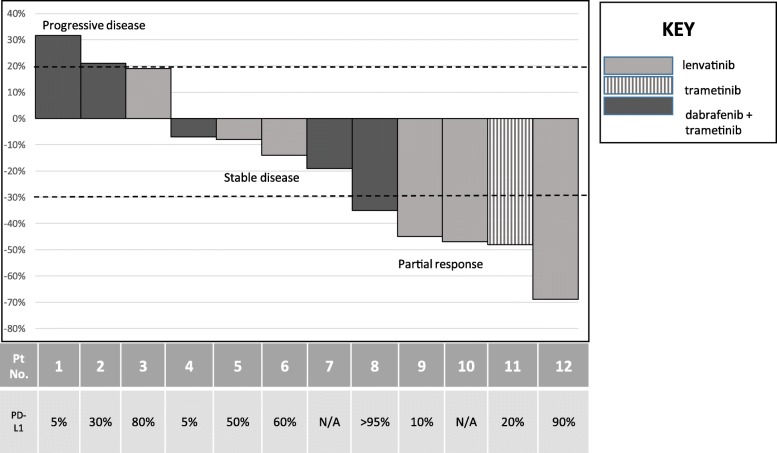
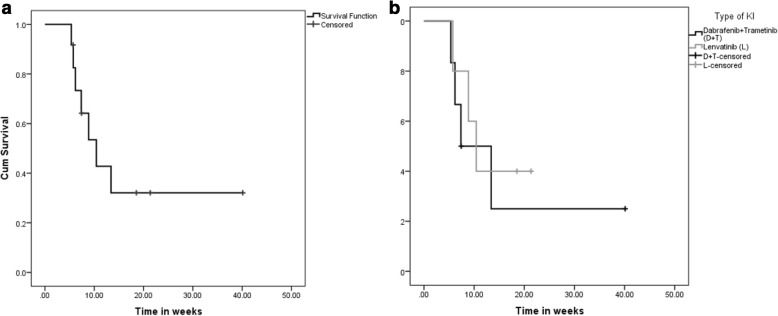
Results: Twelve patients were treated with combination kinase inhibitors plus pembrolizumab at the time of progression on their KI therapy. Median age at initiation of pembrolizumab was 60 years (range 47-84 years). BOR was as follows: 5/12 (42%) had partial response, 4/12 (33%) had stable disease and 3/12 (25%) had progressive disease. Median OS from the start of kinase inhibitor was 10.43 months (95% CI = 6.02, 14.83, range 5.4-40 months). Median OS and PFS from the addition of pembrolizumab were 6.93 months (95% CI = 1.7, 12.15, range 3-15.9 months) and 2.96 months (95% CI = 2.2, 3.7, range 0.57-13.14 months), respectively. Fatigue, anemia and hypertension were the most common AEs encountered on these combinations. Therapy had to be discontinued in 2 patients due to drug induced rash and altered mental status likely from progression of disease.
Conclusion: In a subset of ATC patients, pembrolizumab may be an effective salvage therapy added to kinase inhibitors at the time of progression on these drugs. However, better treatment strategies aimed at incorporating immunotherapy in patients with ATC should be explored. Frontline combination of KI with immunotherapy should be studied in prospective clinical trials.
Keywords: Anaplastic thyroid cancer; Dabrafenib; Immunotherapy; Lenvatinib; Salvage; Thyroid cancer; Trametinib; Undifferentiated.
Conflict of interest statement
Ethics approval and consent to participate
Approved under IRB protocol PA13–0246.
Consent for publication
IRB approved waiver of consent.
Competing interests
Ramona Dadu is on the advisory board of BMS. MEC has received research funding from Eisai and Genentech. NLB has received research funding from Novartis and consulting fees from Eisai. Other authors have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Prasongsook N, Kumar A, Chintakuntlawar AV, Foote RL, Kasperbauer J, Molina J, Garces Y, Ma D, Neben Wittich MA, Rubin J, et al. Survival in response to multimodal therapy in anaplastic thyroid Cancer. J Clin Endocrinol Metab. 2017;102(12):4506–14. - PubMed
-
- Sherman EJ, Lim SH, Ho AL, Ghossein RA, Fury MG, Shaha AR, Rivera M, Lin O, Wolden S, Lee NY, et al. Concurrent doxorubicin and radiotherapy for anaplastic thyroid cancer: a critical re-evaluation including uniform pathologic review. Radiother Oncol. 2011;101(3):425–430. doi: 10.1016/j.radonc.2011.09.004. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials