

Gout prevalence and predictors of urate-lowering therapy use: results from a population-based study
- PMID: 29996922
- PMCID: PMC6042461
- DOI: 10.1186/s13075-018-1633-9
Gout prevalence and predictors of urate-lowering therapy use: results from a population-based study
Abstract
Background: Gout has an increasing global prevalence. Underutilization of urate-lowering therapy (ULT) is thought to be common, via both suboptimal dosing and poor medication adherence. The aims of this study were to determine the prevalence of self-reported gout and the key predictors of ULT use in those with gout in a representative population survey in South Australia.
Methods: Data were obtained from the Spring 2015 South Australian Health Omnibus Survey, a multilevel, systematic, survey in a representative population sample involving face-to-face interviews (n = 3005). This study analyzed responses from respondents aged ≥ 25 years (n = 2531) about self-reported gout, ULT use, sociodemographic factors, lifestyle factors, and comorbidities, using survey weighting. Univariate and subsequent adjusted logistic regression analyses on self-reported gout were performed. ULT use was divided into three categories (never use, prior use, and current use) and these data were analyzed using a multinomial logistic regression model.
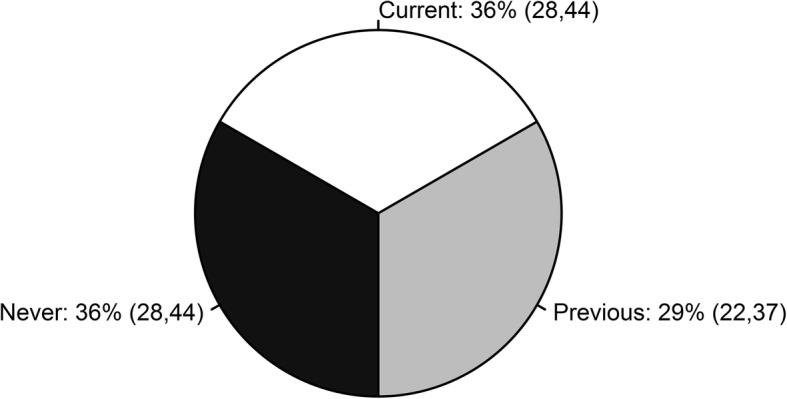
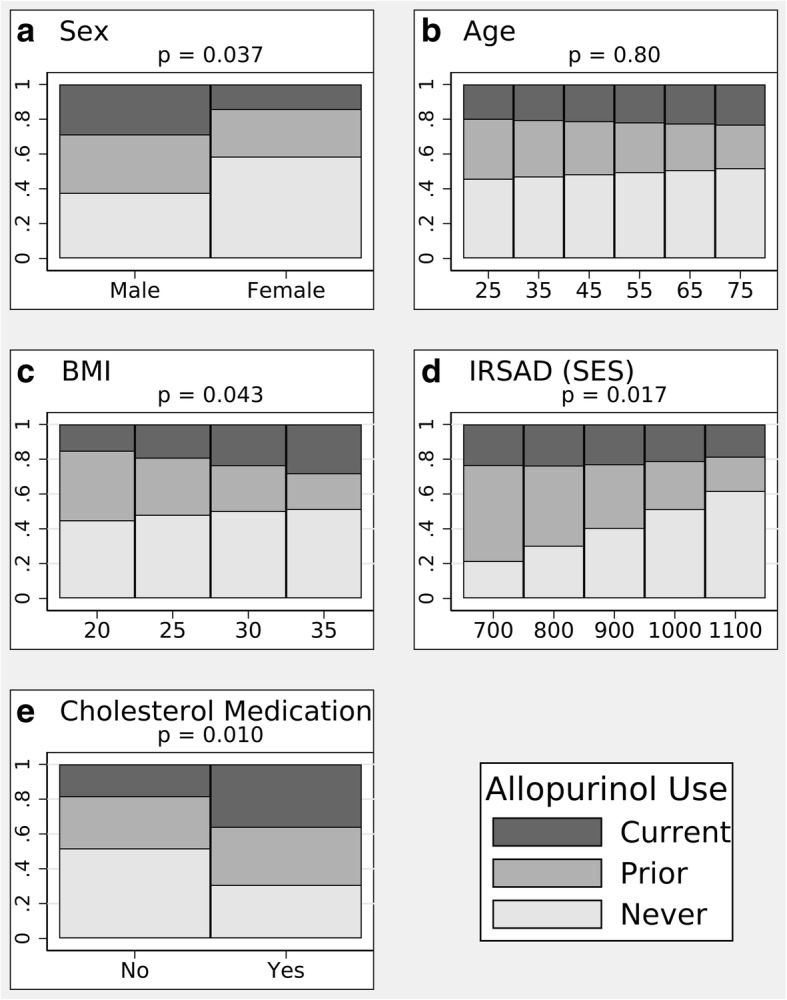
Results: Self-reported gout prevalence was 6.8% (95% CI 5.8, 7.9). The mean age of respondents with gout was 64 years (standard deviation 16) and 82% were male. As expected, older age, male gender, lower socioeconomic status (SES), and higher body mass index (BMI) were associated with gout, as were high alcohol consumption, current smoking, other forms of arthritis, and hypertension or hypercholesterolemia medication, after adjustment for sociodemographic variables. Two thirds of respondents with gout reported ULT use (36% current; 29% previous) with only 55% continuing treatment. Predictors of ULT use included male gender, low SES, and concomitant cholesterol-lowering therapy. Respondents with gout with a higher BMI were more likely to remain on ULT.
Conclusions: Despite gout being a common, potentially disabling joint disease, only 55% of respondents with gout in this study adhered to ULT. Identification of key predictors of ULT use will provide guidance on prescribing strategy in clinical practice and on the quality of gout care in the community.
Keywords: Gout; Population; Predictors; Prevalence; Urate-lowering therapy.
Conflict of interest statement
Ethics approval and consent to participate
This study survey was approved by the Human Research Ethics Committees of the University of Adelaide (project H-097-2010) and the South Australian Department of Health. The study participation was voluntary with verbal informed consent obtained prior to the interview.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
