

Modeling of patient virus titers suggests that availability of a vaccine could reduce hepatitis C virus transmission among injecting drug users
- PMID: 29997251
- PMCID: PMC6552668
- DOI: 10.1126/scitranslmed.aao4496
Modeling of patient virus titers suggests that availability of a vaccine could reduce hepatitis C virus transmission among injecting drug users
Abstract
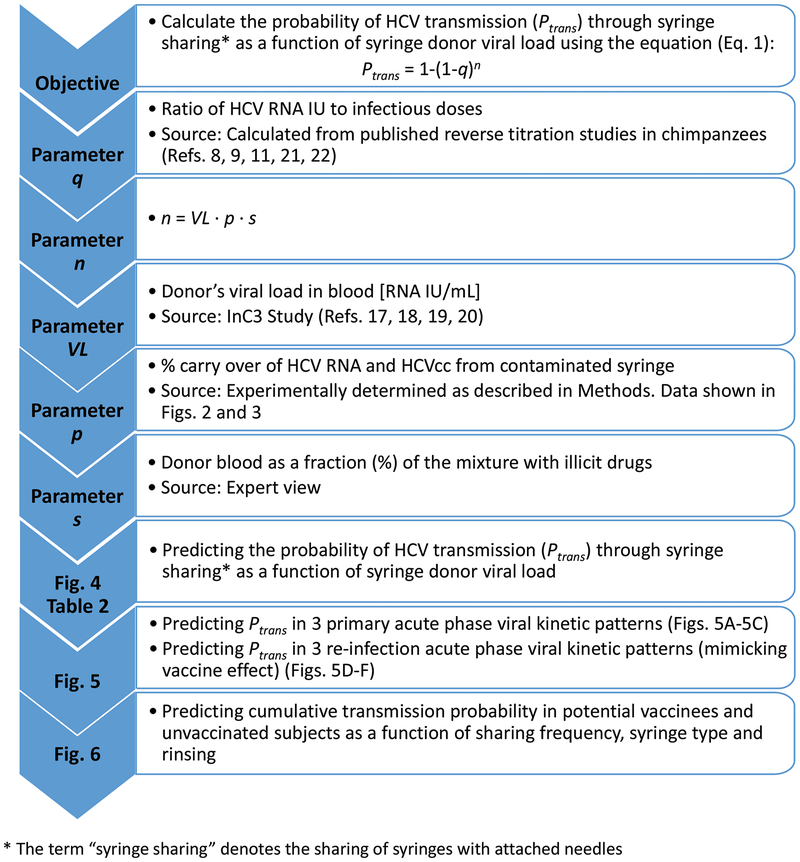
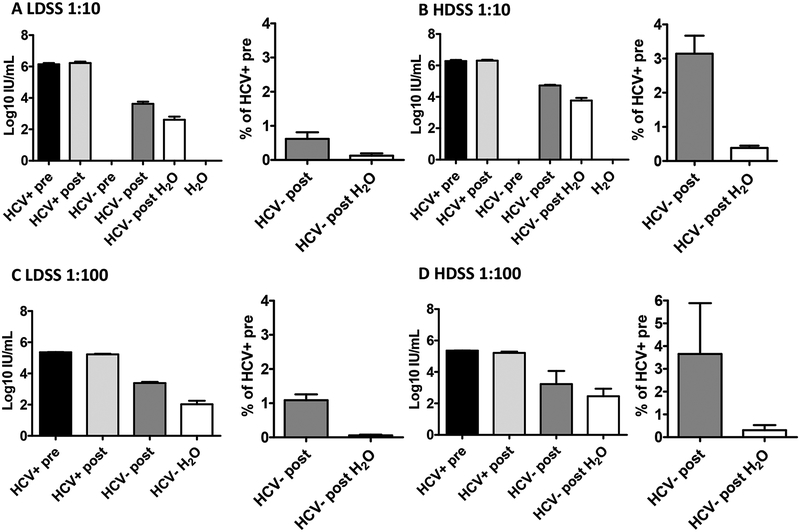
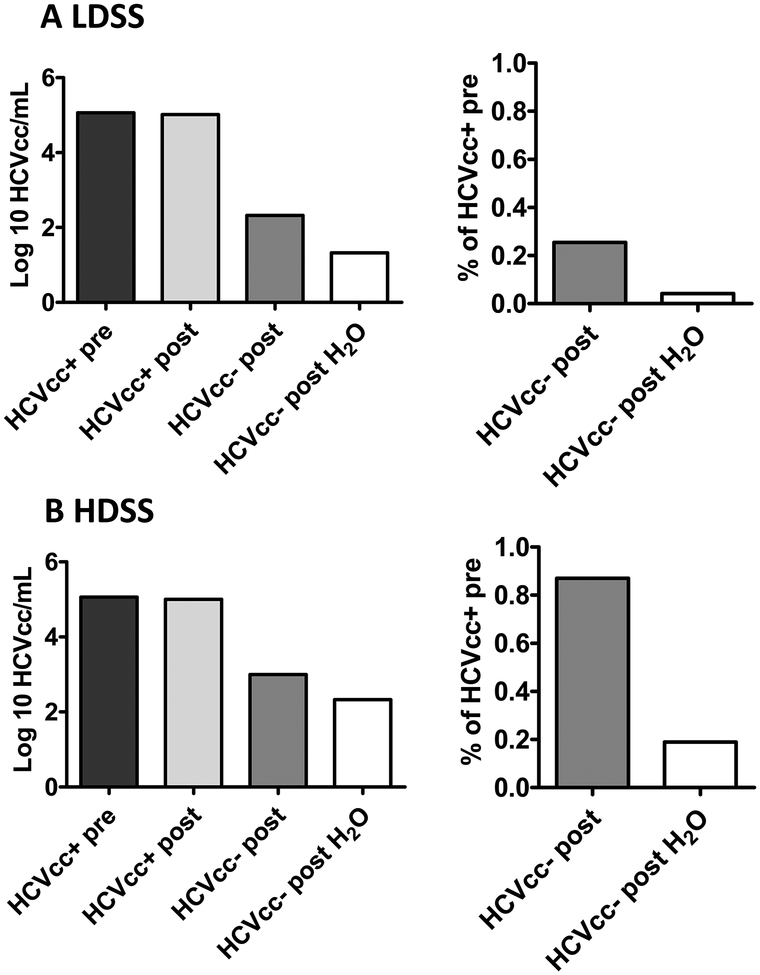
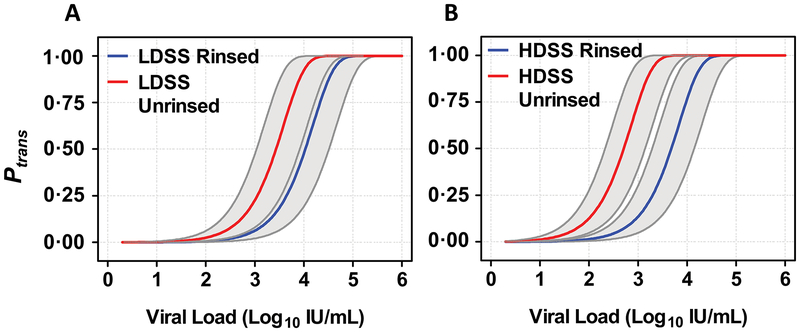
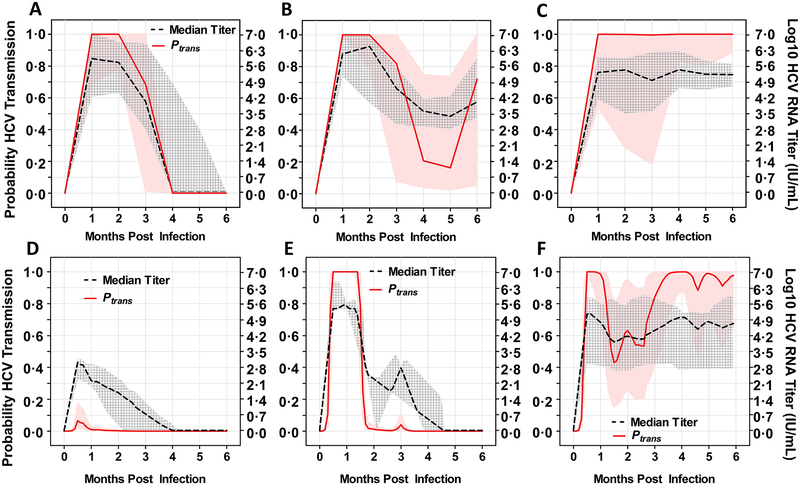
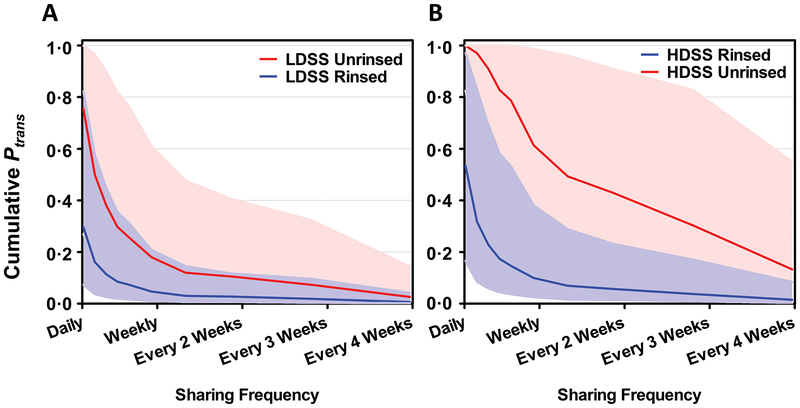
The major route of hepatitis C virus (HCV) transmission in the United States is injection drug use. We hypothesized that if an HCV vaccine were available, vaccination could affect HCV transmission among people who inject drugs by reducing HCV titers after viral exposure without necessarily achieving sterilizing immunity. To investigate this possibility, we developed a mathematical model to determine transmission probabilities relative to the HCV RNA titers of needle/syringe-sharing donors. We simulated sharing of two types of syringes fitted with needles that retain either large or small amounts of fluid after expulsion. Using previously published viral kinetics data from both naïve subjects infected with HCV and reinfected individuals who had previously cleared an HCV infection, we estimated transmission risk between pairs of serodiscordant injecting drug users, accounting for syringe type, rinsing, and sharing frequency. We calculated that the risk of HCV transmission through syringe sharing increased ~10-fold as viral titers (log10 IU/ml) increased ~25-fold. Cumulative analyses showed that, assuming sharing episodes every 7 days, the mean transmission risk over the first 6 months was >90% between two people sharing syringes when one had an HCV RNA titer >5 log10 IU/ml. For those with preexisting immunity that rapidly controlled HCV, the cumulative risk decreased to 1 to 25% depending on HCV titer and syringe type. Our modeling approach demonstrates that, even with transient viral replication after exposure during injection drug use, HCV transmission among people sharing syringes could be reduced through vaccination if an HCV vaccine were available.
Copyright © 2018 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Competing interests
The authors declare that they have no competing interests.
Figures
References
-
- Williams IT, Bell BP, Kuhnert W, Alter MJ, Incidence and transmission patterns of acute hepatitis C in the United States, 1982–2006. Arch Intern Med 171, 242–248 (2011). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
