

Independent risk factors for postoperative AKI and the impact of the AKI on 30-day postoperative outcomes in patients with type A acute aortic dissection: an updated meta-analysis and meta-regression
- PMID: 29997920
- PMCID: PMC6006120
- DOI: 10.21037/jtd.2018.05.47
Independent risk factors for postoperative AKI and the impact of the AKI on 30-day postoperative outcomes in patients with type A acute aortic dissection: an updated meta-analysis and meta-regression
Abstract
Background: This meta-analysis aims to investigate the effects of postoperative acute kidney injury (AKI) on 30-day postoperative outcomes and the independent risk factors for postoperative AKI in patients with type A acute aortic dissection (TAAD).
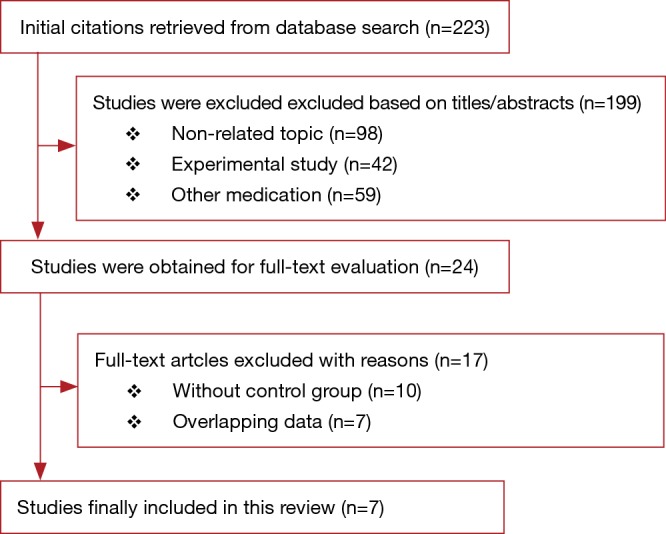
Methods: Relevant reports published between January 1, 2011 and May 31, 2017 were searched in multiple electronic literature databases. A total of seven eligible articles were included in the meta-analysis.
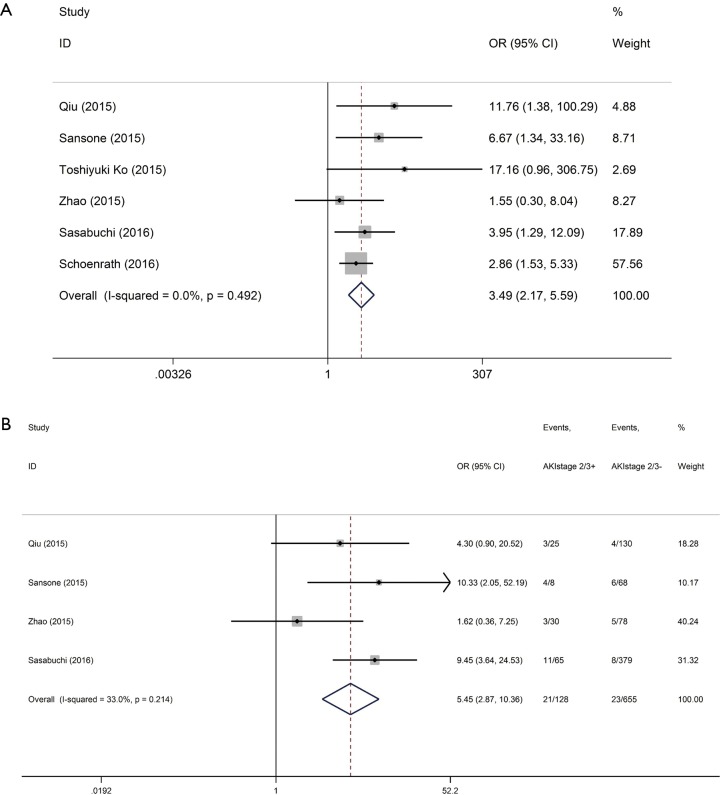
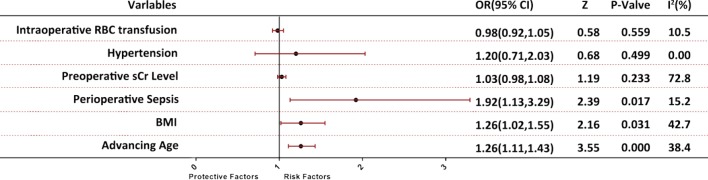
Results: Postoperative AKI was associated with 249% increase in 30-day postoperative mortality [odds ratio (OR): 3.49; 95% confidence interval (CI): 2.17-5.59; P<0.0001]. Subgroup analysis revealed that patients with stage II/III AKI showed 445% increase in 30-day postoperative mortality compared with the control group (OR: 5.45; 95% CI: 2.87-10.36; P<0.0001). Postoperative AKI was also associated with 143%, 432%, and 126% increase in the incidences of 30-day postoperative stroke, bleeding, and respiratory complications, respectively. Notably, high body mass index (BMI), advanced age, and perioperative sepsis were independent risk factors for postoperative AKI in patients with TAAD.
Conclusions: This meta-analysis firstly provided clinical evidence showing the adverse effects of postoperative AKI on 30-day postoperative outcomes in patients with TAAD and identified high BMI, advanced age, and perioperative sepsis as the independent risk factors for postoperative AKI. These findings suggest that preventive or therapeutic methods to effectively manage postoperative AKI may improve 30-day postoperative outcomes in patients with TAAD.
Keywords: 30-day mortality; Acute kidney injury (AKI); postoperative; risk factors; type A acute aortic dissection (TAAD).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources