

ypT0N+: the unusual patient with pathological complete tumor response but with residual lymph node disease after neoadjuvant chemoradiation for esophageal cancer, what's up?
- PMID: 29997939
- PMCID: PMC6006087
- DOI: 10.21037/jtd.2018.04.136
ypT0N+: the unusual patient with pathological complete tumor response but with residual lymph node disease after neoadjuvant chemoradiation for esophageal cancer, what's up?
Abstract
Background: Little is known about the prognostic significance of residual nodal disease in otherwise complete pathologic responders (ypT0N+) after neoadjuvant chemoradiation (nCRT) for esophageal cancer (EC). The purpose is to analyze the long-term outcomes of EC patients with ypT0N+ following nCRT and esophagectomy.
Methods: From a single institution database, 466 consecutive EC patients undergoing esophagectomy after nCRT were collected (1996-2016). ypT0N+ responders were compared to pathological complete responders (ypT0N0) and to pathological non-complete responders (ypT+N0 and ypT+N+).
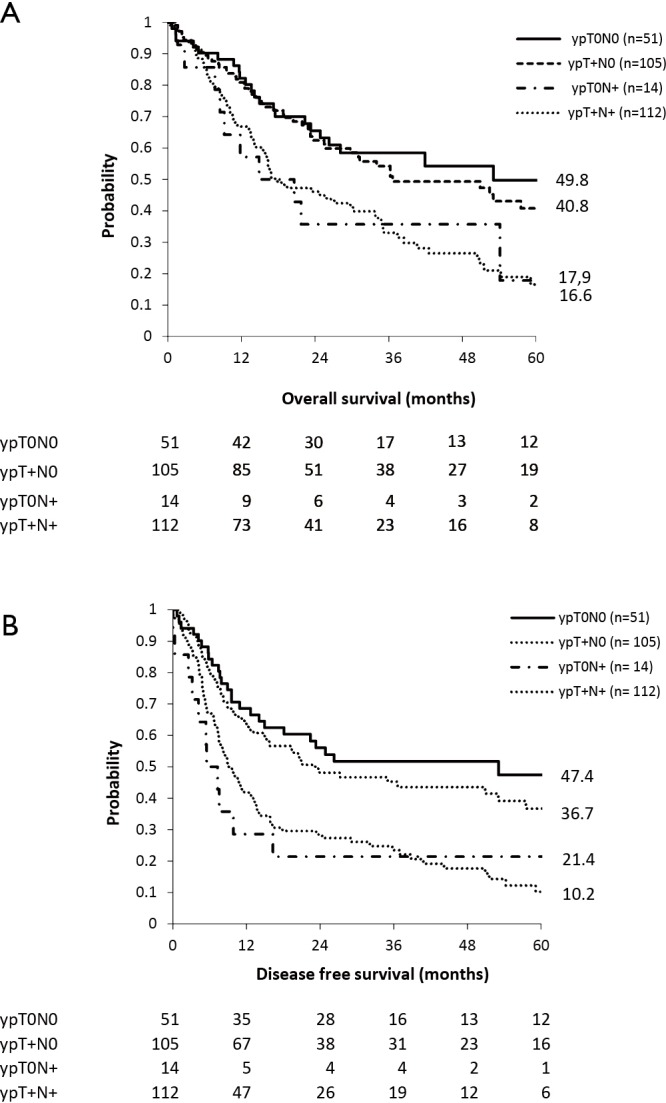
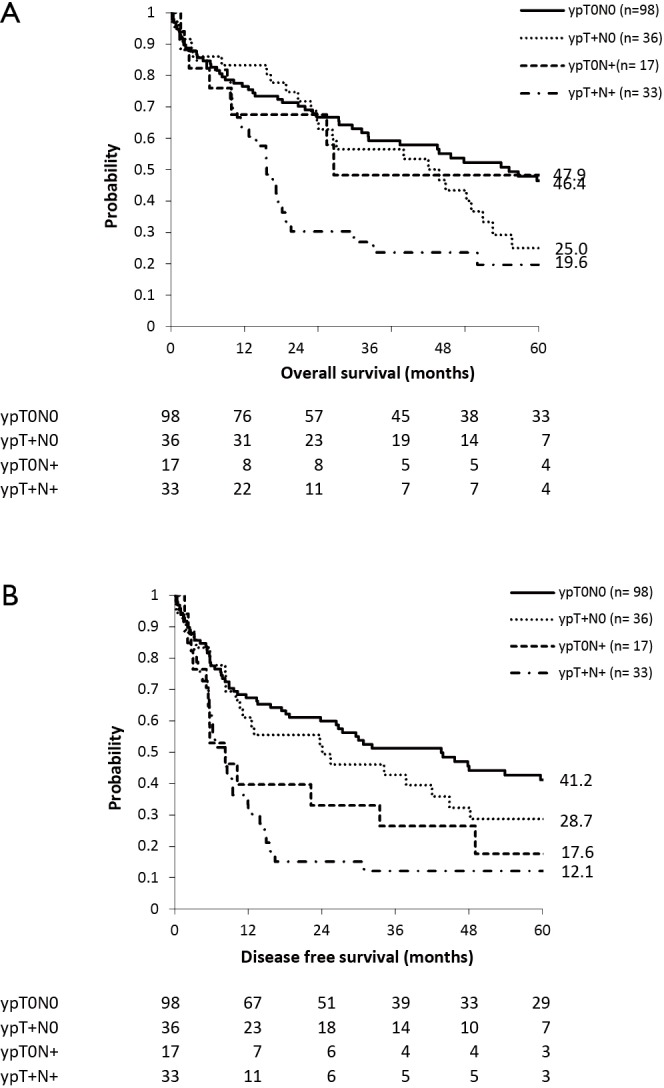
Results: There were 149 ypT0N0, 31 ypT0N+, 141 ypT+N0 and 145 ypT+N+. Median overall survival (OS) was worse in ypT0N+ (21.7 months) and ypT+N+ (16.8 months) compared to ypT0N0 (55.2 months) and ypT+N0 (42.0 months). Stratification by histology revealed a significant difference in prevalence of ypT0: 62.5% in 184 squamous cell carcinomas (SCC) compared to 23.0% in 282 adenocarcinomas (ADC) (P<0.0001) but not in ypT0N+ (15% vs. 22% respectively, P=0.25). In ADC, locoregional recurrence in ypT0N+ (43%) was comparable to ypT+N+ (31%) and more common compared to ypT0N0 (7%) and ypT+N0 (10%), reflected in median OS rates of 20.6, 17.5, 53.0 and 36.6 months respectively. Median OS in ADC is significantly determined by number of positive lymph nodes, being 21.7 months for pN1 and 2.7 months for pN2/3 (P=0.005) in ypT0N+ and 33.7 months for pN1 and 16.2 months for pN2/3 (P=0.031) in ypT+N+. In SCC, locoregional recurrences were found in 17% of ypT0N+, 33% of ypT+N+, 11% of ypT0N0 and 22% in ypT+N0 and median OS was 26.6, 15.6, 55.2 and 43.8 months respectively. In SCC ypN+ number of affected lymph nodes showed no difference on OS.
Conclusions: ypT0N+ in EC patients following nCRT has a poor prognosis and behaves similar to ypT+N+. However, stratification by histology shows that this is especially true in ADC but seems determined by the number of involved lymph nodes.
Keywords: Esophageal neoplasm; neoadjuvant therapy; remission induction; survival analysis.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Schneider PM, Baldus SE, Metzger R, et al. Histomorphologic tumor regression and lymph node metastases determine prognosis following neoadjuvant radiochemotherapy for esophageal cancer: implications for response classification. Ann Surg 2005;242:684-92. 10.1097/01.sla.0000186170.38348.7b - DOI - PMC - PubMed
-
- Depypere L, Moons J, Lerut T, et al. Neoadjuvant chemoradiation treatment followed by surgery for esophageal cancer: there is much more than the mandard tumor regression score. Acta Chir Belg 2016:1-7. [Epub ahead of print]. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous