

Three-field versus two-field lymph node dissection for thoracic esophageal squamous cell carcinoma: a propensity score-matched comparison
- PMID: 29997958
- PMCID: PMC6006065
- DOI: 10.21037/jtd.2018.05.69
Three-field versus two-field lymph node dissection for thoracic esophageal squamous cell carcinoma: a propensity score-matched comparison
Abstract
Background: For the surgery of esophageal cancer, cervical, mediastinal, and abdominal lymph node dissection (three-field lymph node dissection, 3FLND) is still controversial in most countries. This study aims to provide additional evidence of this procedure comparing with mediastinal-abdominal lymph node dissection (two-field lymph node dissection, 2FLND) from a high volume center in China, and also attempts to identify routes to reduce postoperative complications associated with 3FLND.
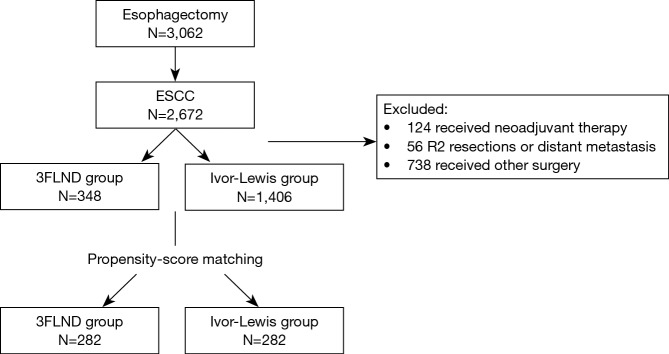
Methods: From January 2009 to December 2013, 348 consecutive patients received esophagectomy with 3FLND and 1,406 patients received Ivor-Lewis with 2FLND in Fudan University Shanghai Cancer Center. After propensity-score matching, 282 pairs of cases without neoadjuvant treatment were selected. Postoperative outcomes and survival of the two groups were analyzed.
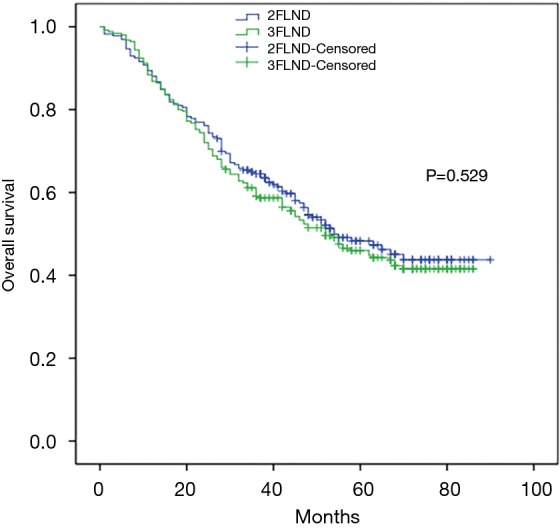
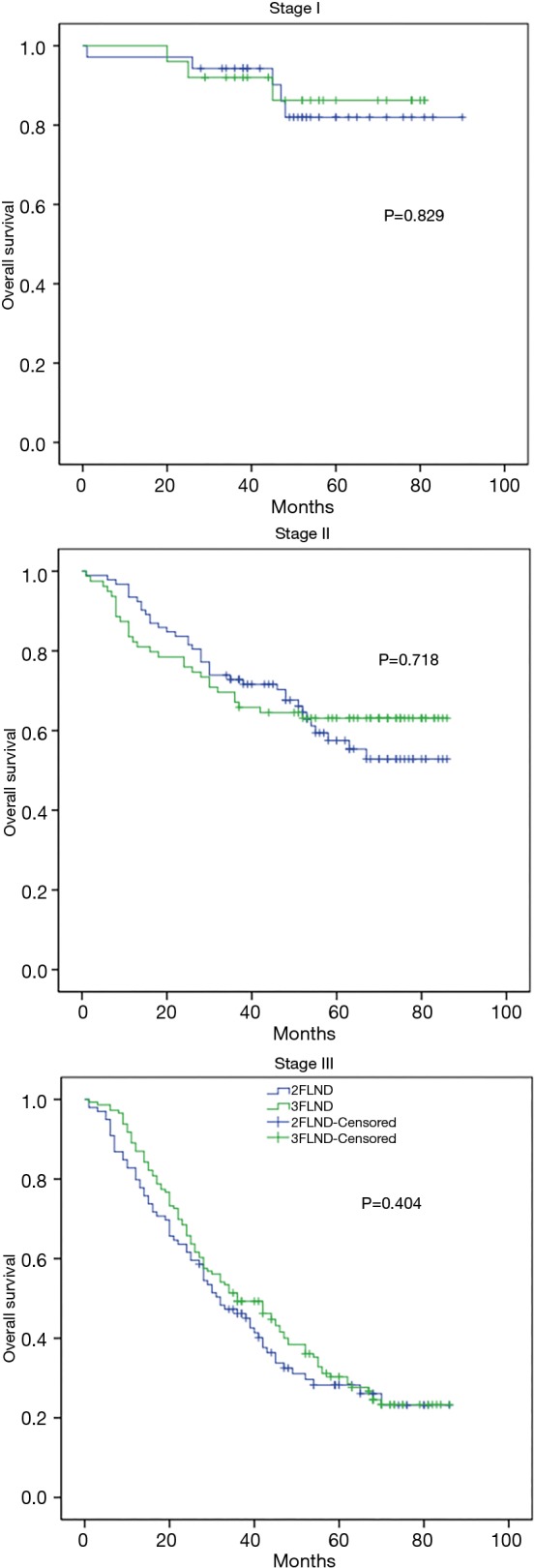
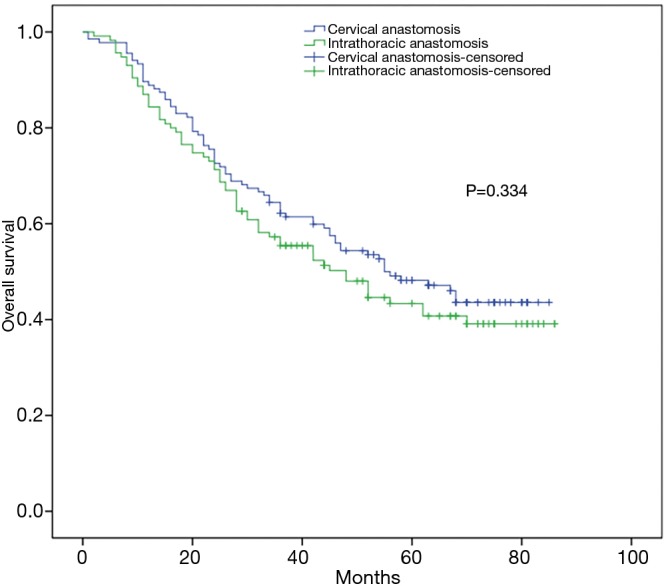
Results: Operative morbidity and mortality rates were 34.8% and 0.4% for 3FLND group; and 25.5% and 0.7% for 2FLND group. Compared with the 2FLND group, the 3FLND group reported more cases of anastomotic leakage (14.9% vs. 4.3%, P<0.001). Multivariate analysis showed that an independent factor of anastomotic leakage was the anastomotic location [HR =0.096 (0.037-0.247), P<0.001] rather than the extent of lymph node dissection. The intrathoracic anastomosis subgroup of 3FLND showed a similar leakage rate as the 2FLND group (4.2% vs. 4.3%). At a median follow-up of 42 months, no significant difference was observed in overall survival between the groups (P=0.529). A subgroup of patients with N1 status who underwent 3FLND showed a better survival trend than those who underwent 2FLND (P=0.093). No significant difference was observed in overall survival between the intrathoracic anastomosis subgroup and cervical anastomosis subgroup (P=0.334).
Conclusions: Intrathoracic anastomosis may reduce the incidence of anastomotic leakage in esophagectomy with 3FLND, with no compromise on overall survival. Compared with the 2FLND, patients with N1 status might benefit more from the 3FLND technique.
Keywords: Esophageal squamous cell carcinoma (ESCC); three-field lymph node dissection (3FLND); two-field lymph node dissection (2FLND).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources