

Nipple sparing mastectomy techniques: a literature review and an inframammary technique
- PMID: 29998077
- PMCID: PMC6006015
- DOI: 10.21037/gs.2017.09.02
Nipple sparing mastectomy techniques: a literature review and an inframammary technique
Abstract
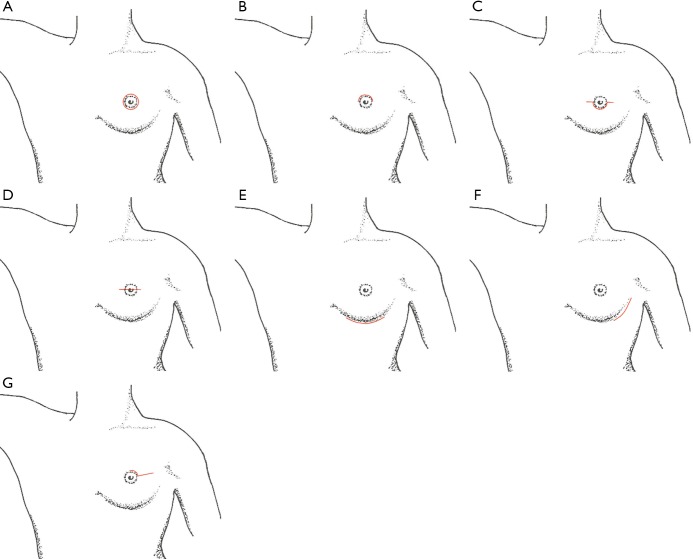
Nipple sparing mastectomy (NSM) has quickly become an accepted technique for patients with selected cancers and for risk reducing surgery. Much of its surgical acceptance over the last decade has been based on the low risk of nipple areolar complex (NAC) occurrence in breast cancer patients. Improved patient satisfaction due to improved cosmetic outcomes with reconstruction have also driven its popularity. We reviewed current English journals to determine the NSM techniques which achieve the lowest complications, best outcomes, and best patient satisfaction. We researched studies showing reductions in complications with improved surgical techniques and patient selection which have been implicated in improved results. In the studies reviewed, incision placement, away from the nipple, resulted in the lowest rates of ischemic nipple complications and the best cosmetic outcomes. The effect of other factors such as surgeon experience and thickness of skin flap development were more difficult to prove. Leaving a 2-3 mm rim of tissue around the nipple bundle was shown to help preserve the nipple vascularity. Lower complication rates with improved outcomes and patient satisfaction were reported in the literature in patients with B or smaller cup sizes, non-smokers, and patients with lower body mass index (BMI). Incision placement, away from the nipple, with preservation of a 2-3 mm rim of tissue around the nipple bundle along with careful patient selection were the most significant variables reviewed which helped to lower complications rates of NSM. Coordinated surgical planning with the breast and plastic surgeons to determine the best surgical approach for each individual patient is necessary to obtain the best results. Although short-term oncologic follow-up seems to be acceptable, longer follow-up will still be needed to define the best breast cancer surgical candidates for the nipple sparing approach.
Keywords: Nipple sparing mastectomy technique; nipple sparing mastectomy complications; nipple sparing mastectomy cosmesis; nipple sparing mastectomy incisions; nipple sparing mastectomy satisfaction; nipple sparing mastectomy vascular supply.
Conflict of interest statement
Conflicts of Interest: Dr. Ashikari is a consultant for LifeCell Corp. The other authors have no conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources