

Comparison of the Safety Planning Intervention With Follow-up vs Usual Care of Suicidal Patients Treated in the Emergency Department
- PMID: 29998307
- PMCID: PMC6142908
- DOI: 10.1001/jamapsychiatry.2018.1776
Comparison of the Safety Planning Intervention With Follow-up vs Usual Care of Suicidal Patients Treated in the Emergency Department
Abstract
Importance: Suicidal behavior is a major public health problem in the United States. The suicide rate has steadily increased over the past 2 decades; middle-aged men and military veterans are at particularly high risk. There is a dearth of empirically supported brief intervention strategies to address this problem in health care settings generally and particularly in emergency departments (EDs), where many suicidal patients present for care.
Objective: To determine whether the Safety Planning Intervention (SPI), administered in EDs with follow-up contact for suicidal patients, was associated with reduced suicidal behavior and improved outpatient treatment engagement in the 6 months following discharge, an established high-risk period.
Design, setting, and participants: Cohort comparison design with 6-month follow-up at 9 EDs (5 intervention sites and 4 control sites) in Veterans Health Administration hospital EDs. Patients were eligible for the study if they were 18 years or older, had an ED visit for a suicide-related concern, had inpatient hospitalization not clinically indicated, and were able to read English. Data were collected between 2010 and 2015; data were analyzed between 2016 and 2018.
Interventions: The intervention combines SPI and telephone follow-up. The SPI was defined as a brief clinical intervention that combined evidence-based strategies to reduce suicidal behavior through a prioritized list of coping skills and strategies. In telephone follow-up, patients were contacted at least 2 times to monitor suicide risk, review and revise the SPI, and support treatment engagement.
Main outcomes and measures: Suicidal behavior and behavioral health outpatient services extracted from medical records for 6 months following ED discharge.
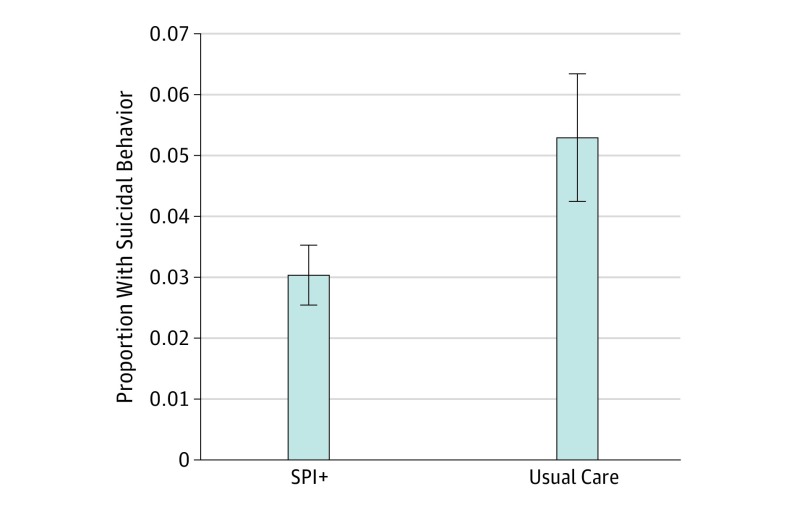
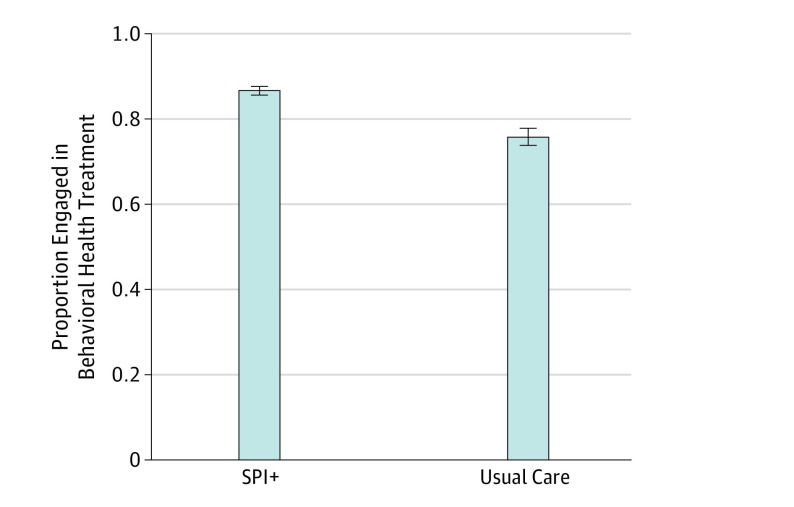
Results: Of the 1640 total patients, 1186 were in the intervention group and 454 were in the comparison group. Patients in the intervention group had a mean (SD) age of 47.15 (14.89) years and 88.5% were men (n = 1050); patients in the comparison group had a mean (SD) age of 49.38 (14.47) years and 88.1% were men (n = 400). Patients in the SPI+ condition were less likely to engage in suicidal behavior (n = 36 of 1186; 3.03%) than those receiving usual care (n = 24 of 454; 5.29%) during the 6-month follow-up period. The SPI+ was associated with 45% fewer suicidal behaviors, approximately halving the odds of suicidal behavior over 6 months (odds ratio, 0.56; 95% CI, 0.33-0.95, P = .03). Intervention patients had more than double the odds of attending at least 1 outpatient mental health visit (odds ratio, 2.06; 95% CI, 1.57-2.71; P < .001).
Conclusions and relevance: This large-scale cohort comparison study found that SPI+ was associated with a reduction in suicidal behavior and increased treatment engagement among suicidal patients following ED discharge and may be a valuable clinical tool in health care settings.
Conflict of interest statement
Figures
References
-
- The Centers for Disease Control and Prevention Leading causes of death reports, national and regional, 1999-2015: web-based injury statistics query and reporting system. https://webappa.cdc.gov/sasweb/ncipc/leadcaus10_us.html. Published 2017. Accessed February 26, 2017.
-
- Office of Mental Health and Suicide Prevention Suicide among veterans and other Americans 2001-2014. https://www.mentalhealth.va.gov/docs/2016suicidedatareport.pdf. Published 2016. Accessed December 5, 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
